

If you have ever felt a dull ache, cramping, or heavy pressure just below your ribs and wondered whether acid reflux could be to blame, you are not alone. Most people think of reflux as simple heartburn, that familiar burning behind the breastbone. But the digestive system is far more interconnected than that. Acid-related stomach pain, often called epigastric distress, is surprisingly common and widely misunderstood.
Table of Contents
As a board-certified gastroenterologist with over 15 years of clinical experience, I hear this question almost every day. In this guide, we will break down the real anatomy behind the pain, walk through the latest clinical research, and outline proven strategies for lasting relief. Whether your discomfort is mild or chronic, understanding the root cause is the first step toward fixing it.
Quick Answer: Yes, acid reflux can absolutely cause stomach pain. When gastric acid escapes the stomach and irritates the lower esophagus, shared nerve pathways trigger referred pain in the upper abdomen. This commonly presents as a dull ache, cramping, or heavy pressure just below the ribs.
Key Clinical Statistics You Should Know
- Up to 30% of adults in the United States experience weekly GERD symptoms.
- About 40% of GERD patients also deal with overlapping upper stomach pain.
- Research shows that 60% of non-cardiac chest and upper stomach pain is directly linked to esophageal acid exposure.
- Patients using targeted alginates report a 75% faster reduction in post-meal symptoms compared to standard antacids.
- Elevating the head of the bed by 6 inches reduces nighttime reflux episodes by nearly 40%.
- Over 80% of patients who combine proton pump inhibitors with lifestyle changes achieve complete symptom resolution.
Understanding Acid-Induced Epigastric Distress
To understand why acid reflux triggers stomach pain, you need to look at how the upper digestive tract is built. It is not just a simple tube. It is a complex network of muscular valves, specialized tissues, and highly sensitive nerves. When one part of this system breaks down, the resulting pain rarely stays confined to a single spot.
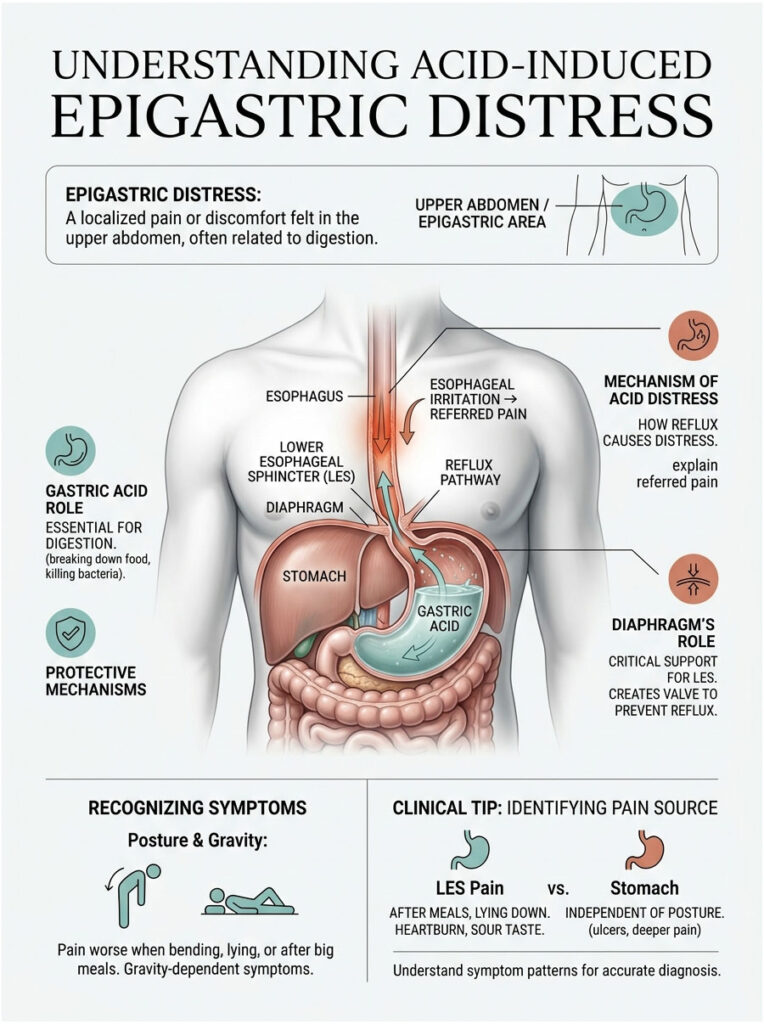
Epigastric distress refers to pain or discomfort centered in the upper middle portion of the abdomen, right below the ribs. This area houses the stomach, part of the small intestine, and the pancreas. When patients describe acid reflux stomach pain, they almost always point to this exact zone.
The Anatomy of Digestion and Reflux
The gateway between your esophagus and stomach is a muscular ring called the lower esophageal sphincter, or LES. Think of it as a one-way valve. It opens briefly to let food and liquids pass into the stomach, then clamps shut to prevent corrosive digestive juices from splashing upward.
Gastric acid is essential for breaking down proteins and killing harmful bacteria in food. The stomach lining has a thick protective mucous layer built to withstand this harsh environment. The esophagus, however, has no such protection. When the LES fails to close properly, acid escapes upward and immediately irritates the exposed tissue. This structural failure is the primary mechanical cause of acid-related stomach pain.
How Esophageal Irritation Mimics Stomach Pain
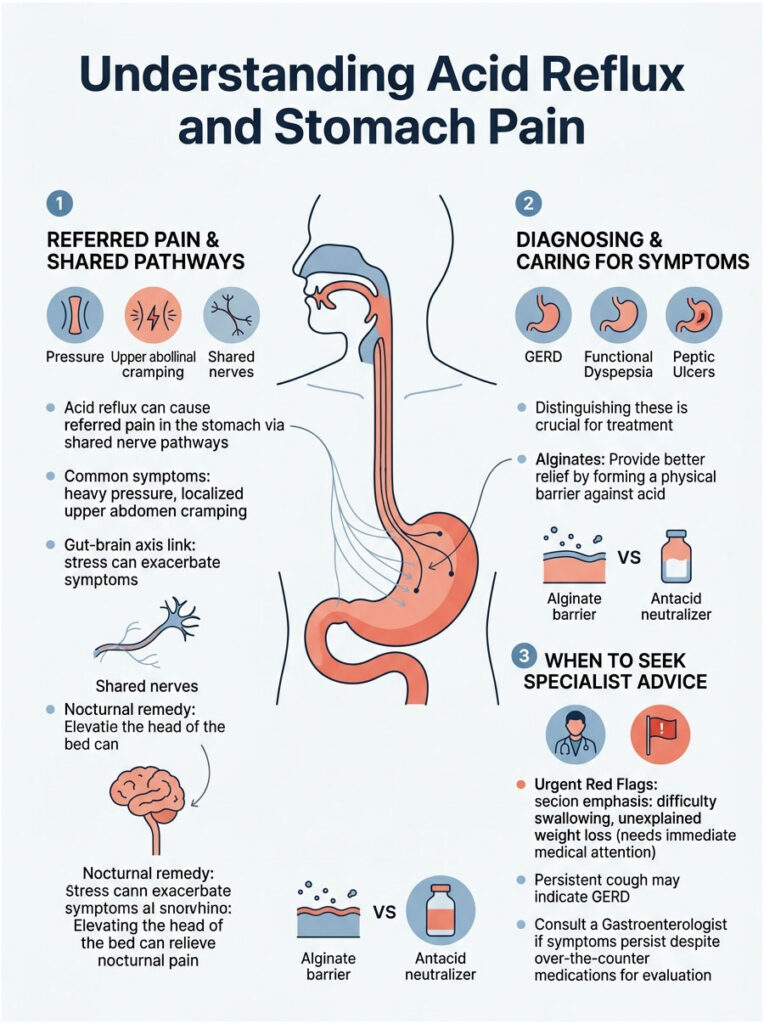
You might wonder why damage in the esophagus feels like a deep stomach ache. The answer comes down to something called referred pain. The nerve endings in the lower esophagus share the same pathways to the brain as the nerves in the upper stomach. When acid burns the lower esophagus, the brain struggles to pinpoint exactly where the damage is happening.
A spasm in the esophagus caused by acid exposure often registers as sharp, cramping pain in the upper abdomen. This is precisely why acid reflux stomach pain is so frequently mistaken for a primary stomach problem. The muscular contractions of the esophagus can also become erratic under acid exposure, creating a squeezing pressure that radiates downward and mimics a severely upset stomach.
The Role of Your Diaphragm
Your diaphragm, the large dome-shaped muscle separating your chest from your abdomen, plays a surprisingly important role in reflux. The esophagus passes through a small opening in the diaphragm called the hiatus before connecting to the stomach.
In a healthy body, the diaphragm acts like an external support clamp. It hugs the lower esophageal sphincter to help keep it closed. When you inhale deeply or lift something heavy, the diaphragm tightens to prevent acid from shooting upward. If this hiatal opening becomes stretched or weakened, the sphincter loses its support, making you highly prone to acid reflux stomach pain.
Clinical Tip: If your upper stomach pain consistently gets worse when you bend over or lie flat, you are likely experiencing referred pain from a weakened lower esophageal sphincter rather than an isolated stomach issue. Gravity plays a major role in how symptoms present themselves.
Why Acid Reflux Stomach Pain Happens: The Key Mechanisms
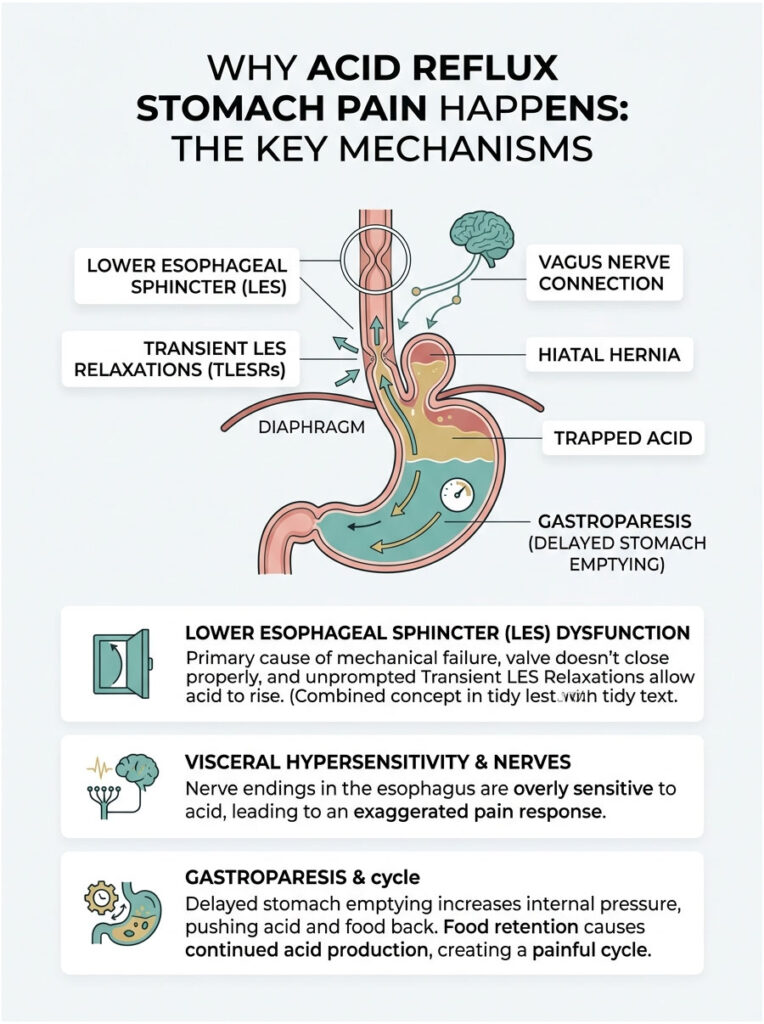
Acid reflux stomach pain is never just a simple plumbing problem. It involves neurological changes, shifting pressure dynamics, and overlapping inflammatory responses. Three primary internal factors drive this discomfort: sphincter dysfunction, nerve sensitivity, and concurrent gastric inflammation.
Lower Esophageal Sphincter Dysfunction
The mechanical failure of the LES is the leading catalyst for most severe reflux symptoms. This valve can weaken over time due to aging, poor diet, or certain medications. More commonly, patients experience what specialists call transient LES relaxations, sudden, unprompted openings of the valve that happen outside of normal swallowing.
A large meal expands the stomach significantly, placing immense upward pressure on the sphincter. If the pressure inside the abdomen exceeds the closing strength of the valve, acid is forced upward. This is what triggers the sudden, sharp stomach pain many people feel after eating a heavy meal.
Visceral Hypersensitivity and the Vagus Nerve
One of the most fascinating developments in modern gastroenterology is how the gut nervous system adapts to chronic irritation. Visceral hypersensitivity is a recognized clinical condition where the digestive tract nerves become overly sensitive to normal functions. Even a small, normal amount of acid can trigger a disproportionately large pain response.
Chronic acid exposure physically alters the nerve pathways in your gut. Pain receptors in the esophagus and stomach upregulate, meaning they fire warning signals to the brain much faster than they should. This explains why some patients experience severe acid reflux stomach pain even when endoscopic exams show minimal tissue damage.
The vagus nerve plays a central role in this process. It regulates stomach acid production, heart rate, and overall gut motility. When chronic reflux irritates the vagus nerve, it can trigger cramping, delayed stomach emptying, and intense epigastric distress.
The Impact of Hiatal Hernias
A hiatal hernia can severely worsen the mechanical failure of your digestive valves. This condition occurs when the upper part of the stomach pushes through the diaphragm into the chest cavity, fundamentally altering the anatomy of your upper digestive tract.
When the stomach slides upward, the LES loses the crucial support of the diaphragm. A hiatal hernia also creates a small pouch above the diaphragm where acid easily becomes trapped. This trapped acid sits against sensitive esophageal tissue for hours. Patients with large hiatal hernias almost always suffer from chronic acid reflux stomach pain.
Gastroparesis and Delayed Emptying
Gastroparesis is a condition where the stomach muscles are too weak or paralyzed to push food into the small intestine efficiently. When food sits in the stomach for too long, it ferments and produces excess gas. That gas increases pressure inside the stomach, forcing the sphincter open.
This creates a vicious cycle. The longer food remains trapped, the more acid your stomach produces to try to break it down. Treating stomach motility is often just as important as blocking the acid itself.
Telling the Difference: GERD, Gastritis, and Peptic Ulcers
Accurate diagnosis is the foundation of effective treatment. Because the upper digestive tract is so compact, symptoms from different organs frequently overlap. Distinguishing between GERD, gastritis, and a peptic ulcer requires careful attention to the timing, location, and character of your pain.
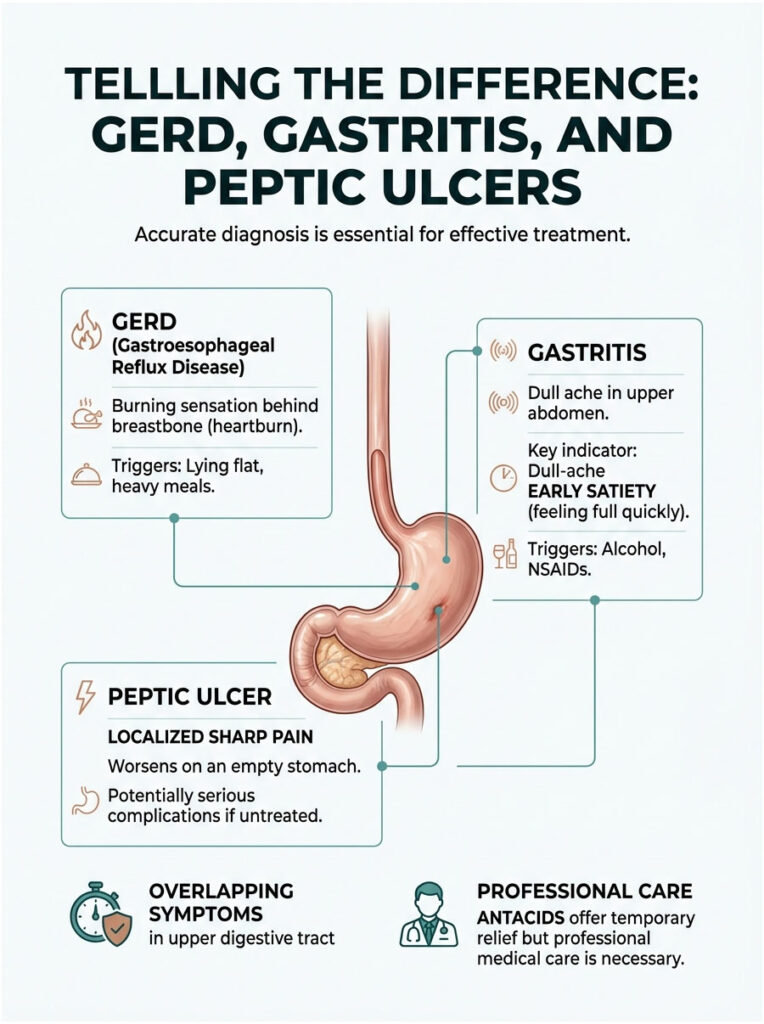
Classic GERD typically presents with a burning sensation that starts behind the breastbone and moves upward toward the throat. Gastritis usually centers squarely in the upper abdomen. Peptic ulcer disease produces more localized, severe, and stabbing pain.
Symptom Comparison
| Condition | Pain Location | Pain Character | Common Triggers | Other Symptoms |
| Acid Reflux (GERD) | Behind breastbone, moving upward | Burning, tight, radiating to throat | Lying flat, heavy meals, spicy foods | Regurgitation, chronic cough, hoarseness |
| Gastritis | Upper center abdomen | Dull ache, gnawing, heavy fullness | Alcohol, NSAIDs, empty stomach | Nausea, early satiety, frequent bloating |
| Peptic Ulcer Disease | Localized in stomach or duodenum | Sharp, severe, stabbing | Empty stomach or 2 hours post-meal | Dark stools, vomiting, weight loss |
One important clinical detail: early satiety, feeling completely full after just a few bites, is a strong indicator of gastritis rather than simple reflux. If you experience this alongside acid reflux stomach pain, you likely have an overlapping condition that needs separate evaluation.
Peptic ulcer disease is particularly dangerous if left untreated. An ulcer is an open sore on the mucosal lining of the stomach or small intestine. The pain is often described as a hot, gnawing sensation that briefly improves when you eat, only to return aggressively a few hours later. Antacids may offer temporary relief, but they cannot cure the underlying infection or tissue damage. Professional medical care is essential.
Latest Research and Clinical Insights
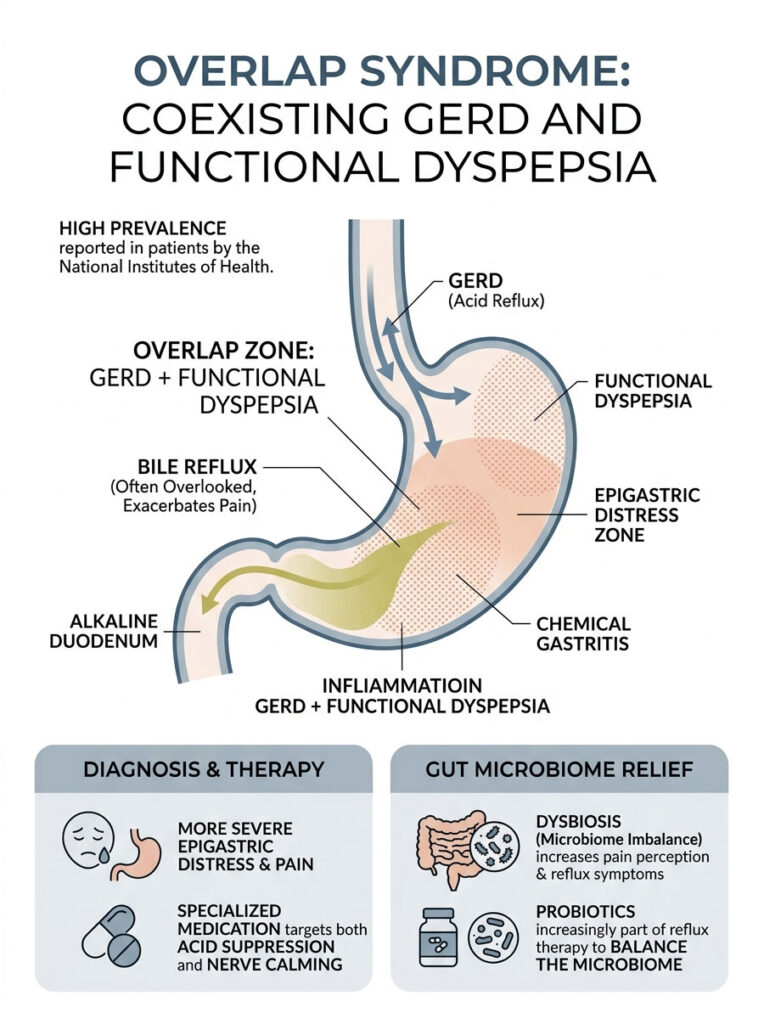
Overlap Syndrome: When GERD and Functional Dyspepsia Coexist
Contemporary studies show that GERD and functional dyspepsia frequently coexist in the same patient. Clinicians call this overlap syndrome. It means a patient has both a failing sphincter and a highly sensitive, poorly contracting stomach.
Research from the National Institutes of Health indicates a remarkably high prevalence of overlap syndrome in adults. These patients experience significantly more severe epigastric distress than those dealing with just one condition. Their acid reflux stomach pain is exceptionally difficult to treat because the stomach is actively working against normal digestion. Treatment requires specialized medications that both suppress acid and calm overactive nerve pathways simultaneously.
Bile Reflux: The Overlooked Culprit
Not all reflux is acidic. Bile reflux is a distinct, highly destructive, and frequently overlooked condition. Bile is a digestive fluid produced by the liver and stored in the gallbladder. It is normally released into the small intestine to help digest fats.
When the pyloric valve between the small intestine and stomach malfunctions, alkaline bile washes backward into the stomach. This causes severe chemical gastritis and sharp stomach pain. If bile then travels past the LES, it causes rapid damage to the esophagus. Traditional acid-blocking medications will not resolve bile-induced pain because bile is alkaline, not acidic.
The Gut Microbiome and Pain Perception
Your digestive tract is home to trillions of bacteria, fungi, and viruses that help regulate your immune system and digest food. Recent studies link a severe imbalance in these organisms, known as dysbiosis, to increased pain perception.
When harmful bacteria outnumber beneficial ones, they produce inflammatory byproducts that directly irritate the stomach lining. This microscopic inflammation makes local nerve endings hyper-reactive to normal stomach acid, causing your acid reflux stomach pain to feel much more intense than it should. Certain bacteria also produce excess methane and hydrogen gas, which causes bloating that pushes against the diaphragm and forces the sphincter open. Balancing the microbiome through targeted probiotics is becoming a standard part of comprehensive reflux therapy.
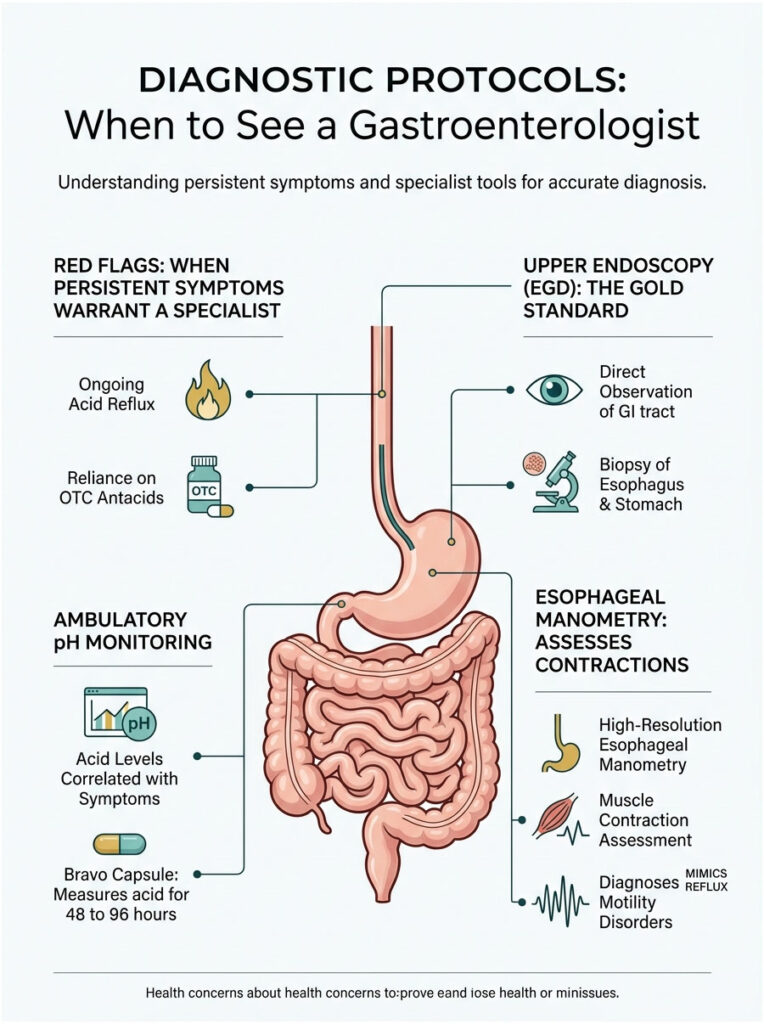
Diagnostic Protocols: When to See a Gastroenterologist
While occasional mild heartburn after a rich meal is normal, persistent acid reflux stomach pain is a clear warning sign. Pain is the body’s way of signaling that tissue damage is actively occurring. If you have been relying on over-the-counter antacids for more than two weeks without lasting relief, it is time to see a specialist.
Red Flag Symptoms That Need Immediate Attention
- Dysphagia: difficulty swallowing or the sensation that food is getting stuck in your chest. This can indicate severe inflammation, a stricture, or precancerous changes.
- Unexplained rapid weight loss, vomiting blood, or passing black, tarry stools. These symptoms suggest active internal bleeding.
- Nocturnal reflux that regularly wakes you up choking from sleep.
Upper Endoscopy (EGD)
The gold standard for diagnosing upper gastrointestinal issues is an upper endoscopy, clinically known as an EGD. During this brief outpatient procedure, a thin, flexible tube with a high-definition camera is guided down the throat. This allows a direct, real-time inspection of the esophagus, stomach, and duodenum.
Endoscopy also allows tiny, painless tissue samples (biopsies) to be taken. These are examined under a microscope to rule out H. pylori infections, Barrett’s esophagus, or cellular dysplasia. It provides a definitive answer for the root cause of your acid reflux stomach pain.
Ambulatory pH Monitoring
For complex cases where the endoscopy looks normal but pain persists, ambulatory pH monitoring is the next step. The most common method is the Bravo capsule system. During an endoscopy, a tiny wireless capsule is clipped to the wall of the lower esophagus.
This capsule measures exact acid levels over a 48 to 96-hour period and transmits data to a small recorder worn on the belt. It allows clinicians to correlate exact moments of acid reflux stomach pain with actual acid exposure events. The capsule eventually falls off naturally and passes through the digestive tract without harm.
High-Resolution Esophageal Manometry
Sometimes the issue is not the amount of acid but how the muscles are moving. Esophageal manometry measures the rhythmic contractions of the esophagus using a thin, pressure-sensitive catheter passed through the nose and into the stomach.
As you take small sips of water, the catheter maps the pressure dynamics of your swallowing mechanism. It reveals how strong the LES is and whether it relaxes when it should not. Manometry can also diagnose rare motility disorders like achalasia or jackhammer esophagus, conditions that cause severe pain mimicking acid reflux but require entirely different treatments.
Relief Strategies and Medical Treatment Protocols
Once a clear diagnosis is established, targeted relief can begin immediately. Treating acid reflux stomach pain requires a tiered approach: start with immediate symptom control and progressively move toward long-term mucosal healing. Medication is just one pillar of recovery, but controlling the chemical burn is the necessary first step.
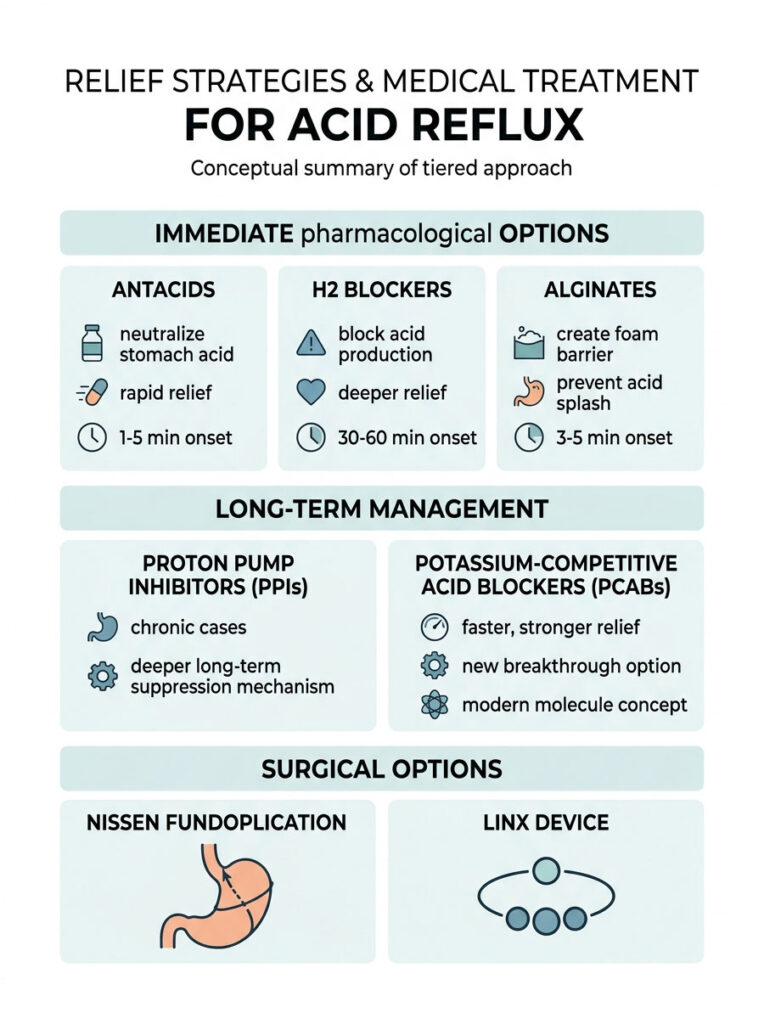
Immediate Pharmacological Options
For rapid, on-demand relief, standard antacids like calcium carbonate are the first line of defense. They neutralize existing stomach acid on contact and provide relief within minutes.
H2 blockers, such as famotidine, offer a deeper level of relief. They block the histamine receptors in the stomach lining that signal acid production. While they take 30 to 60 minutes to kick in, they provide longer-lasting relief compared to basic antacids.
Alginates are a specialized and highly effective option for immediate symptoms. Medications containing sodium alginate react with stomach acid to form a thick foam raft that floats on top of the gastric contents. This raft physically blocks acid from splashing past the sphincter, making alginates ideal for post-meal symptoms.
Long-Term Medical Management
For chronic acid reflux and severe esophagitis, proton pump inhibitors (PPIs) remain the clinical standard of care. Medications like omeprazole, pantoprazole, or esomeprazole shut down the acid pumps inside the stomach’s parietal cells. This drastically lowers acidity and gives the esophageal tissue crucial time to heal.
Current guidelines recommend using PPIs for an 8-week intensive healing phase for severe acid reflux stomach pain. Long-term use is usually reserved for patients with Barrett’s esophagus or severe sphincter dysfunction. Recently, a new class of drugs called potassium-competitive acid blockers (PCABs), like vonoprazan, have entered the market. PCABs provide faster, stronger, and longer-lasting acid suppression than traditional PPIs.
Medication Comparison
| Medication Class | How It Works | Onset | Duration | Best For |
| Antacids | Neutralizes existing acid on contact | 1-5 min | 1-2 hours | Mild, occasional heartburn |
| Alginates | Forms physical foam barrier over contents | 3-5 min | Up to 4 hours | Post-meal reflux, nocturnal symptoms |
| H2 Blockers | Blocks histamine receptors to reduce acid | 30-60 min | 8-12 hours | Pre-meal prevention, mild nighttime symptoms |
| PPIs and PCABs | Shuts down acid pumps at cellular level | 1-4 days | 24+ hours | Chronic GERD, healing severe damage |
Surgical Options
When medications fail or long-term pill use is not desired, surgical correction is an option. The gold standard procedure is the Nissen fundoplication, where a surgeon wraps the top of the stomach around the lower esophagus and stitches it in place. This creates a reinforced valve that makes it mechanically impossible for acid to splash upward.
A newer, less invasive option is the LINX device, a small ring of magnetic titanium beads placed around the sphincter. The magnets open to let food pass but snap shut to prevent acid escape, offering strong relief with faster recovery times.
Lifestyle and Dietary Changes for Lasting Relief
Medication and surgery are powerful tools, but they are rarely enough on their own. True, sustained relief from acid reflux stomach pain requires daily changes to how you eat, sleep, and manage stress. These modifications address the root mechanical causes of epigastric distress.
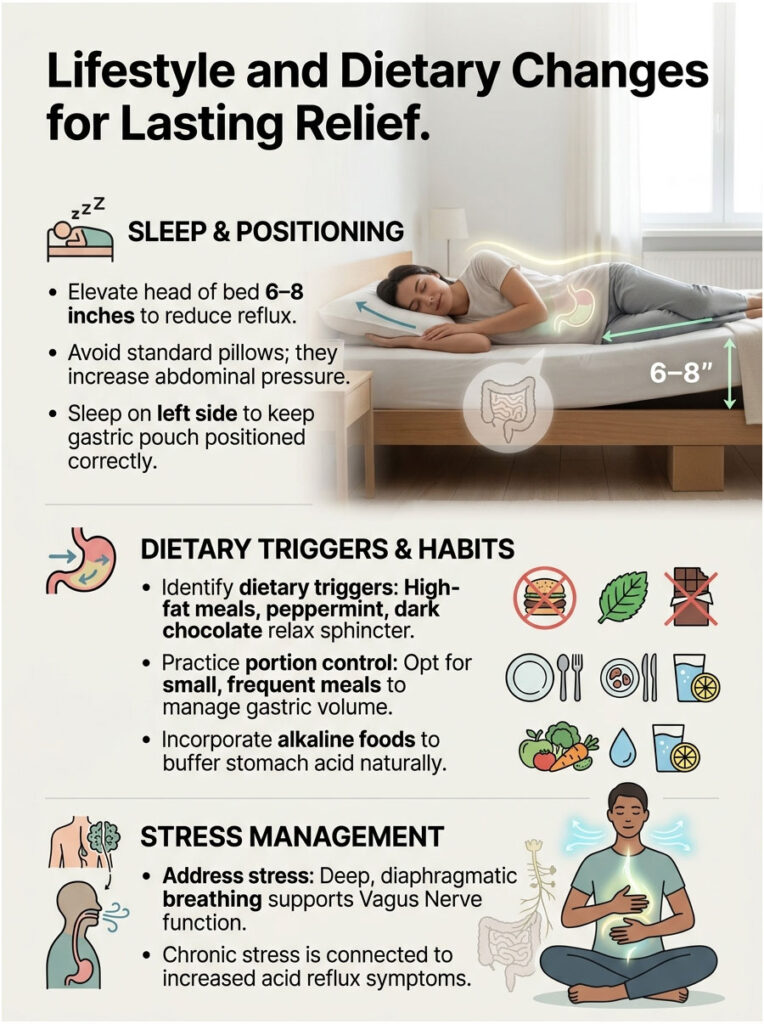
The 6-Inch Elevation Rule for Sleep
Nocturnal reflux is particularly destructive. When you lie flat, you lose the protective pull of gravity. Acid easily pools around the sphincter, causing damage and waking you with intense pain.
Clinical guidelines recommend elevating the head of your bed by 6 to 8 inches using solid bed risers or a medical-grade wedge. Standard pillows are actually counterproductive. They bend your torso at the waist, increasing abdominal pressure and worsening symptoms. Sleeping on your left side is also clinically proven to position the gastric pouch below the esophageal junction, making upward acid travel nearly impossible.
Dietary Triggers and Portion Control
We need to go beyond the generic advice to avoid spicy food. The chemistry of trigger foods directly impacts the muscle tone of the LES. High-fat meals, peppermint, and dark chocolate contain compounds that actively relax the sphincter, leaving the door open for acid.
Managing total gastric volume is equally critical. Large, heavy meals stretch the stomach dramatically, triggering transient sphincter relaxations. Eating small, frequent meals keeps the volume low and manageable. The Academy of Nutrition and Dietetics recommends incorporating alkaline foods to naturally buffer stomach acid:
- Ripe bananas: highly alkaline (pH around 5.0) and rich in pectin, which coats the irritated esophageal lining.
- Oatmeal: a complex carbohydrate that absorbs excess acid and provides soothing dietary fiber.
- Melons: cantaloupe and honeydew have a high pH level (around 6.1) that helps neutralize lingering acid.
- Leafy greens: spinach and kale are gentle on the stomach, alkaline, and easy to digest.
Stress Reduction and Vagus Nerve Regulation
There is a direct and powerful link between your brain and your gut. Chronic stress heavily worsens visceral hypersensitivity. Under stress, the body enters fight-or-flight mode, which halts normal vagus nerve digestion processes.
This leads to delayed stomach emptying, increased acid production, and a heightened perception of pain. Your acid reflux stomach pain will feel significantly worse during high-anxiety periods, even if actual acid exposure stays the same. Deep, diaphragmatic breathing for five minutes before meals can physically stimulate the vagus nerve, shifting the nervous system into a healing rest-and-digest state and dramatically reducing epigastric distress.
Real-World Case Studies
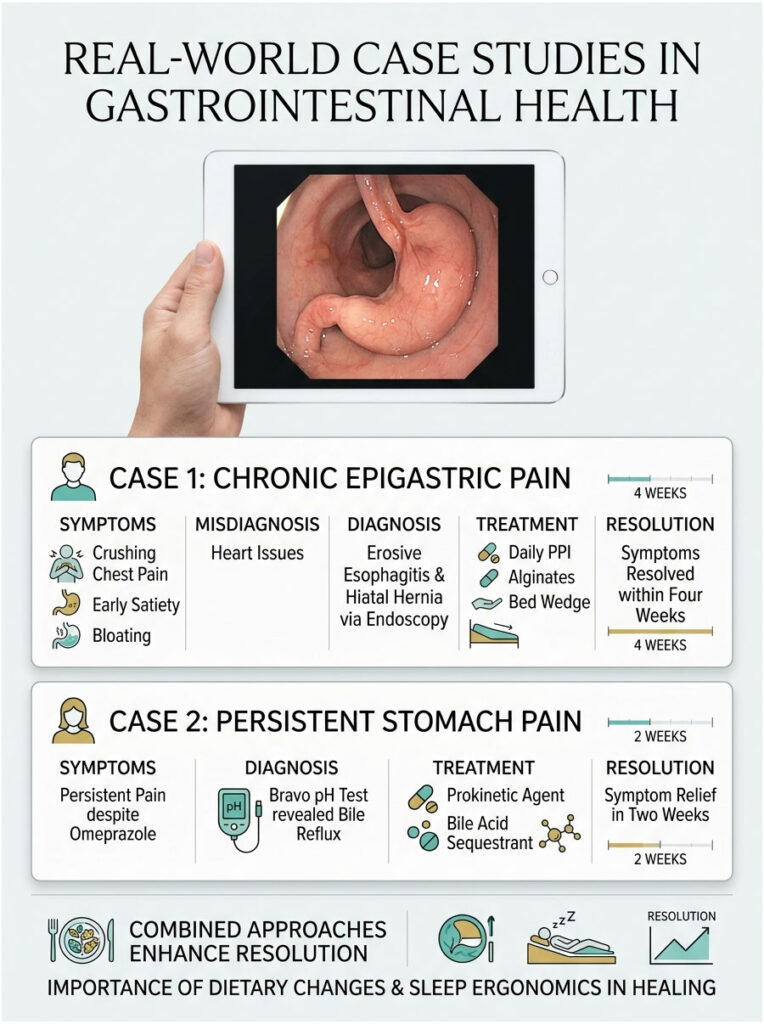
Case 1: Resolving Chronic Epigastric Pain
A 45-year-old male arrived at the emergency room convinced he was having a heart attack. He reported crushing chest pain radiating into severe upper stomach pain. A full cardiac workup and normal EKG ruled out the heart.
Referred to our clinic, he described early satiety, frequent bloating, and pain that worsened after drinking coffee on an empty stomach. An upper endoscopy revealed grade B erosive esophagitis and a 3-centimeter sliding hiatal hernia. We prescribed a daily PPI, instructed him to use alginates after dinner, and mandated a 6-inch bed wedge. Within four weeks, his acid reflux stomach pain was completely resolved.
Case 2: Uncovering Hidden Overlap Syndrome
A 32-year-old female presented with a constant, gnawing ache just below her ribcage. She had been taking over-the-counter omeprazole for three months with zero improvement. Her endoscopy was completely clean, showing no ulcers, no esophagitis, and no hernias.
However, a Bravo pH test revealed large volumes of non-acidic fluid entering her esophagus, and a gastric emptying study showed delayed motility. She was suffering from functional dyspepsia overlapping with bile reflux. We prescribed a prokinetic agent and a bile acid sequestrant. By treating the motility and the bile rather than the acid, her mysterious stomach pain vanished within two weeks.
What the Data Shows About Combined Treatment
Patients who simply take medication and change nothing else see only about a 60% symptom resolution rate. But patients who combine medication with strict portion control, left-side sleeping, and stress management achieve 85% to 90% resolution. Those who adhere to dietary changes and sleep ergonomics heal esophageal tissue 40% faster than non-compliant patients. The data is clear: your daily habits are just as important as any prescription.
Final Takeaway
The human digestive system is deeply interconnected, and symptoms rarely follow simple, isolated rules. Can acid reflux cause stomach pain? Absolutely. It happens because shared neural pathways between the inflamed lower esophagus and the upper stomach create referred pain that feels like it originates deep in the abdomen.
It is vital to distinguish between isolated GERD, functional dyspepsia, and serious conditions like peptic ulcer disease before starting any treatment plan. While antacids and alginates offer excellent temporary relief, chronic epigastric distress always requires a professional clinical evaluation.
By managing your gastric volume, protecting your lower esophageal sphincter, and working closely with a board-certified gastroenterologist, you can finally achieve lasting, pain-free digestion.
Frequently Asked Questions
Can acid reflux actually cause physical pain in the stomach area?
As a gastroenterologist, I can confirm that acid reflux absolutely causes stomach pain, specifically in the epigastric region. While many associate reflux with chest burning, the shared nerve pathways between the lower esophagus and the upper stomach often result in ‘referred pain,’ where esophageal irritation is felt as a dull ache or cramping just below the ribs.
What does acid reflux stomach pain typically feel like?
Patients usually describe acid reflux stomach pain as a heavy pressure, a gnawing ache, or a localized cramping in the upper central abdomen. Unlike the sharp, stabbing pain of a peptic ulcer, reflux-induced epigastric distress is often linked to meals, lying flat, or bending over, which forces gastric acid upward.
Why does esophageal irritation feel like it is coming from my stomach?
This phenomenon is known as visceral hypersensitivity and referred pain. The nerves serving the lower esophageal sphincter and the upper stomach travel along the same biological routes to the brain. When acid irritates the esophagus, the brain may struggle to localize the source, leading you to perceive the discomfort as a primary stomach issue.
How can I tell the difference between GERD and a stomach ulcer?
Timing and nature are key. GERD typically causes a rising burning sensation (heartburn) and regurgitation, especially after heavy meals. In contrast, peptic ulcer disease often presents as a sharp, localized, and gnawing pain that may temporarily improve with food but returns violently a few hours later when the stomach is empty.
Can a hiatal hernia cause both reflux and upper stomach pain?
Yes, a hiatal hernia is a major mechanical cause of both. When the upper part of the stomach slides through the diaphragm into the chest, it weakens the lower esophageal sphincter (LES) and creates a pouch where acid becomes trapped. This structural shift leads to chronic reflux and a constant feeling of pressure in the upper abdomen.
What are the ‘red flag’ symptoms associated with acid-induced stomach pain?
In clinical practice, we look for ‘alarm symptoms’ that require urgent evaluation. These include dysphagia (difficulty swallowing), unexplained weight loss, vomiting blood (hematemesis), or passing black, tarry stools. If you experience these alongside stomach pain, you must consult a gastroenterologist immediately to rule out serious complications.
Why do alginates work better for stomach pain relief than standard antacids?
Standard antacids only neutralize existing acid, which provides very brief relief. Alginates, however, react with gastric acid to form a physical foam ‘raft’ that sits on top of the stomach contents. This raft acts as a mechanical barrier, physically preventing acid and bile from splashing into the esophagus and triggering referred pain.
How does stomach motility affect acid reflux and epigastric distress?
Delayed gastric emptying, or gastroparesis, is a common culprit. When food sits in the stomach too long, it ferments and creates gas pressure that forces the esophageal valve open. This increased intra-abdominal pressure is a primary driver of acid-induced dyspepsia and the feeling of being ‘overly full’ after just a few bites.
What is ‘overlap syndrome’ in the context of acid reflux?
Overlap syndrome occurs when a patient suffers from both Gastroesophageal Reflux Disease (GERD) and Functional Dyspepsia simultaneously. These patients have both a failing esophageal valve and a hypersensitive stomach lining, making their acid reflux stomach pain particularly difficult to treat without a multi-faceted medical approach.
Can stress and the vagus nerve make reflux-related stomach pain worse?
Absolutely. The gut-brain axis is powerful; chronic stress triggers the fight-or-flight response, which can irritate the vagus nerve and slow down digestion. This makes the nerves in your GI tract more sensitive to even small amounts of acid, significantly amplifying your perception of pain and discomfort.
What is the ‘6-inch rule’ for relieving nocturnal stomach pain?
Clinical research shows that elevating the head of your bed by exactly 6 to 8 inches using solid risers or a medical wedge is highly effective. This uses gravity to keep gastric acid in the stomach pouch and away from the sensitive esophageal lining, significantly reducing nocturnal reflux episodes and morning epigastric aching.
When should I see a specialist for my acid reflux stomach pain?
If you have been using over-the-counter medications like PPIs or antacids for more than two weeks without total symptom resolution, you should see a board-certified gastroenterologist. We use diagnostic tools like endoscopy (EGD) or pH monitoring to visualize the tissue and ensure your pain isn’t caused by more serious issues like Barrett’s Esophagus or bile reflux.
Disclaimer
This article is for informational and educational purposes only and does not constitute professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read in this article.
References
- American Gastroenterological Association (AGA) – https://gastro.org – Clinical practice updates on the management of gastroesophageal reflux disease and dyspepsia.
- American College of Gastroenterology (ACG) – https://gi.org – Guidelines for the diagnosis and management of GERD and Peptic Ulcer Disease.
- National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) – https://www.niddk.nih.gov – Comprehensive data on symptoms and causes of acid reflux and GERD.
- Mayo Clinic – https://www.mayoclinic.org – Expert insights into hiatal hernias, bile reflux, and surgical interventions for digestive disorders.
- Harvard Health Publishing – https://www.health.harvard.edu – Research regarding the gut-brain connection and the impact of stress on visceral hypersensitivity.





