

Americans spend roughly $10 billion a year on over-the-counter cold products, and a staggering number of us grab the wrong one. I’ve watched friends dose themselves with NyQuil for a runny nose (zero fever in sight), chug DayQuil while already on extra-strength Tylenol (hello, liver stress), and swear by phenylephrine pills the FDA officially declared useless in 2024.
Table of Contents
Colds are common. Smart cold treatment isn’t. This guide fixes that, one symptom at a time.

| Quick Answer Pick cold medicine by symptom, not by combo pack. Use ibuprofen or acetaminophen for fever and aches, pseudoephedrine or a steroid spray for congestion, guaifenesin for a wet cough, dextromethorphan for a dry cough, and a non-drowsy antihistamine like Claritin for a runny nose. Skip oral phenylephrine; the FDA confirmed it doesn’t work. |
| At a Glance • Match the medicine to the symptom; never double up on the same active ingredient • The FDA’s 2024 advisory confirmed oral phenylephrine is ineffective as a decongestant • NSAIDs outperform acetaminophen for inflammation but carry stomach and kidney risks • People with high blood pressure should avoid pseudoephedrine • Adults get 2 to 3 colds per year; most resolve in 7 to 10 days (CDC) • Red flags: fever above 101.3°F for 3+ days, symptoms past 10 days, shortness of breath • Zinc lozenges started within 24 hours of first symptoms may shorten a cold slightly |
Why Most Americans Grab the Wrong Cold Medicine
Walk down the cold-and-flu aisle at any CVS or Walgreens and you’ll see the problem instantly. Forty different boxes, half of them purple-blue, all promising “multi-symptom relief.” Reading the active ingredient list feels like reading a contract, so most folks grab what they’ve used before.

I’ve watched this play out in pharmacies for years. People pick NyQuil because a cousin swears by it, not because it matches what’s actually wrong with them. That’s how you end up taking an antihistamine you don’t need, a cough suppressant that stops a cough you should be coughing out, and a pain reliever that was already in the Excedrin you took two hours ago.
The Multi-Symptom Combo Trap
Combination products like Theraflu, Mucinex Fast-Max, and Alka-Seltzer Plus typically bundle four active ingredients into one dose. That’s fine if you truly have all four symptoms. If you don’t, you’re treating problems that aren’t there while stacking side effects.
The biggest offender is acetaminophen. It’s in Tylenol, in DayQuil, in Theraflu, in Mucinex Fast-Max, and in dozens of other products. Combine two of those on the same day and you can blow past the FDA’s 4,000 mg daily limit fast. Liver damage from accidental acetaminophen overdose is more common than people realize.
What the 2024 FDA Phenylephrine Ruling Actually Means
In September 2024, an FDA advisory committee ruled that oral phenylephrine, the decongestant in most “PE” products like Sudafed PE, Benadryl Allergy Plus Congestion, and many DayQuil variants, doesn’t work when swallowed. Your stomach breaks it down before it reaches your nose.
I had a neighbor tell me she’d been taking Sudafed PE for a decade and “getting nothing out of it.” The research now explains why. Pseudoephedrine (real Sudafed, sold behind the pharmacy counter) still works. Topical phenylephrine in nasal sprays also still works. Oral PE pills, though, can go in the trash.
Stat snapshot: The CDC estimates adults in the US average 2 to 3 colds annually and children average 6 to 10. Colds cause roughly 22 million missed school days per year, and the NIH pegs the nation’s annual total at around 1 billion colds. This isn’t a rare condition; it’s a national habit.
Cold Medicine by Symptom: The Complete Matching Chart
Here’s the matrix I wish every pharmacy would print and hang on the wall. Identify your most disruptive symptom, find the row, ignore the rest of the aisle.
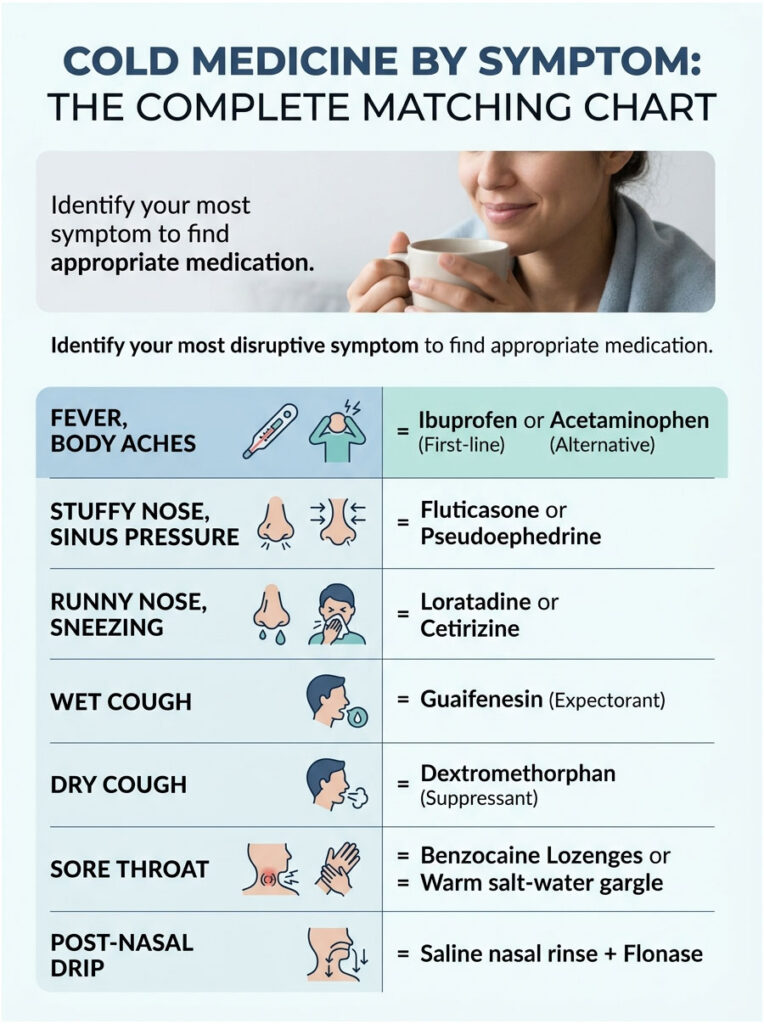
Table 1: Cold Medicine by Symptom Matcher
| Your Symptom | First-Line OTC Pick | Alternative | Avoid If You… |
| Fever, body aches, chills | Ibuprofen (Advil, Motrin) 400–600 mg every 6 hours | Acetaminophen (Tylenol) 650–1,000 mg every 6 hours | Have kidney disease, ulcers, or take blood thinners (NSAIDs); have liver disease (Tylenol) |
| Stuffy nose, sinus pressure | Fluticasone (Flonase) 1–2 sprays per nostril daily | Pseudoephedrine (Sudafed) 30–60 mg every 4–6 hours | Have high blood pressure, glaucoma, or heart rhythm issues |
| Runny nose, sneezing | Loratadine (Claritin) 10 mg daily | Cetirizine (Zyrtec) 10 mg daily | Have severe kidney disease (reduce dose) |
| Wet, productive cough | Guaifenesin (Mucinex) 600–1,200 mg every 12 hours | Hydration + warm fluids | Have severe nausea (guaifenesin worsens it) |
| Dry, hacking cough | Dextromethorphan (Delsym) 60 mg every 12 hours | Honey, 1–2 teaspoons (adults and kids over 1) | Take SSRIs or MAOIs (serotonin interaction) |
| Sore throat | Benzocaine lozenges (Cepacol) or warm salt-water gargle | Ibuprofen for swelling | Have a history of methemoglobinemia (benzocaine) |
| Post-nasal drip | Saline nasal rinse + Flonase | First-generation antihistamine at night | Have recent sinus surgery (check first) |
Fever, Body Aches, and Chills
When you’re burning up and your joints feel like they belong to someone twice your age, you want an NSAID. Ibuprofen and naproxen (Aleve) reduce the inflammation driving both the fever and the muscle pain. Mayo Clinic lists them as mainstays for cold symptom relief.
Acetaminophen works too, but it only lowers fever and blunts pain; it doesn’t touch inflammation. In practice, I tell people with garden-variety aches to start with ibuprofen if their stomach tolerates it, and switch to Tylenol only if NSAIDs are off-limits. Aspirin works for adults, but never give aspirin to anyone under 19 because of Reye syndrome risk. That’s a hard rule.
Nasal Congestion and Sinus Pressure
Real Sudafed (pseudoephedrine) still works, and it’s still available, but you have to show ID at the pharmacy counter thanks to the Combat Methamphetamine Epidemic Act. It can raise blood pressure and keep you awake, so daytime use is smarter than bedtime.
Steroid nasal sprays like Flonase, Nasacort, and Rhinocort take 12 to 48 hours to reach full effect but deliver strong, focused anti-inflammatory action right where you need it. I’ve seen these quietly outperform oral decongestants for sinus-heavy colds, especially in people with a history of allergies.
Oxymetazoline nasal spray (Afrin) gives fast relief, but never use it more than three consecutive days. Rebound congestion (rhinitis medicamentosa) is a real and annoying problem to reverse.
Runny Nose and Sneezing
Antihistamines shine here. Second-generation options (Claritin, Zyrtec, Allegra) cause little to no drowsiness. First-generation ones (Benadryl, Chlor-Trimeton) dry things up more aggressively but will knock most adults out.
I’ve had friends tell me Benadryl at bedtime was “the only thing that let me sleep” during a cold, and that’s often true. The tradeoff: next-day grogginess and, in long-term use, emerging evidence of cognitive risk in older adults.
Wet Cough vs. Dry Cough
This is where cold medicine by symptom logic matters most. A wet cough bringing up mucus is useful; it’s clearing your lungs. Don’t suppress it. Use an expectorant like guaifenesin to thin the mucus and drink water like it’s your job.
A dry, tickly cough that won’t let you sleep is a different beast. That’s when dextromethorphan (Delsym, Robitussin DM) earns its keep. Take it at night, not during a productive daytime cough.
Understanding the 6 Main Cold Medicine Categories
You’ll feel less lost in the aisle once you know what each class does. In practice, cold relief comes from six tools, not forty.
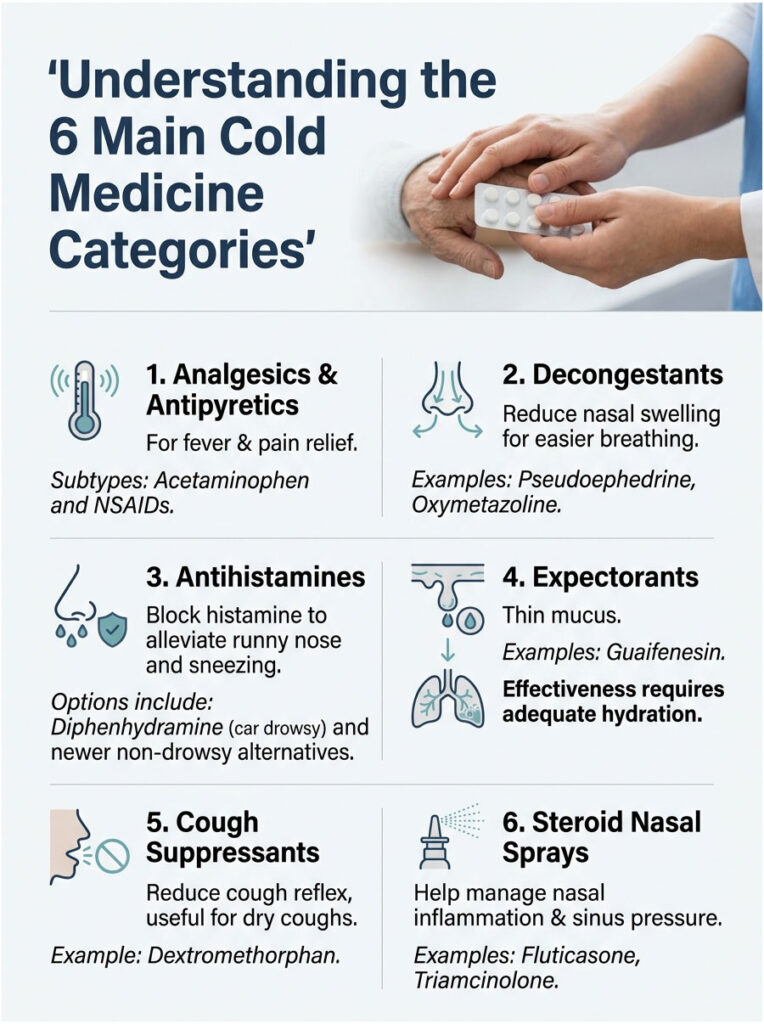
1. Analgesics and Antipyretics
These handle fever, headache, and body aches. Two subtypes matter: acetaminophen (Tylenol), which is easy on the stomach but hard on the liver at high doses; and NSAIDs (ibuprofen, naproxen, aspirin), which tackle inflammation but can irritate the stomach and stress kidneys.
2. Decongestants
Decongestants shrink swollen nasal tissue so you can breathe. Pseudoephedrine (oral) and oxymetazoline (spray) are the workhorses. Phenylephrine pills are out; phenylephrine sprays still work.
3. Antihistamines
These block histamine, the chemical that makes your nose run and your eyes itch. Useful for cold-related runny nose and sneezing, especially at night. Diphenhydramine (Benadryl) is old-school; loratadine, cetirizine, and fexofenadine are the modern non-drowsy options.
4. Expectorants
Guaifenesin is basically the only player. It thins mucus so you can cough it up. Only works if you stay hydrated; without fluids, it does nothing.
5. Cough Suppressants
Dextromethorphan (DXM) dulls the cough reflex by acting on the brainstem. Useful at night or for a dry cough. Avoid if you take SSRIs, MAOIs, or certain mood medications (serotonin syndrome risk).
6. Steroid Nasal Sprays
Fluticasone, triamcinolone, and budesonide calm inflammation directly in the nasal lining. They’re not instant, but they’re my go-to recommendation for anyone whose cold turned into sinus pressure lasting more than a couple days.
Drug Combinations: What’s Safe, What’s Dangerous
Drug stacking is where colds turn into ER visits. Let’s make this simple.
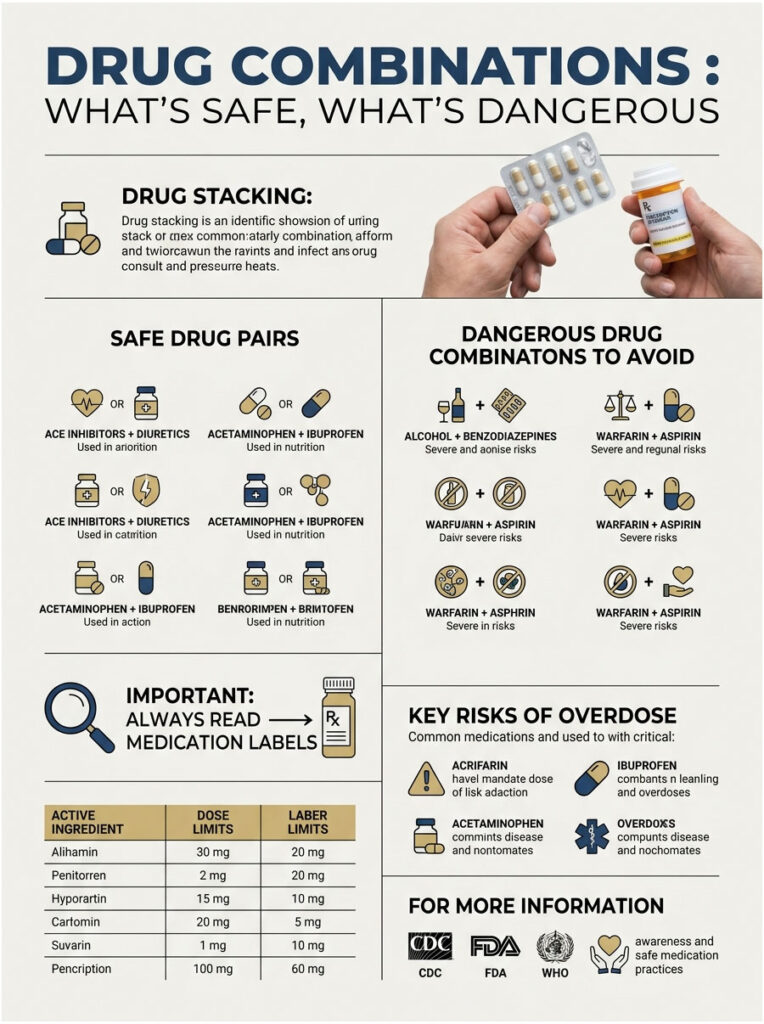
Safe Pairs
- Ibuprofen + acetaminophen: Yes. You can alternate every 3 to 4 hours for stubborn fever. AAFP guidance supports this.
- Mucinex + Sudafed: Yes. Different mechanisms, no overlap.
- Flonase + oral antihistamine: Yes. Works well for sinus-allergy overlap.
- Tylenol + Delsym: Yes. Pain relief plus cough suppression.
Dangerous Doubles
- Tylenol + DayQuil/NyQuil/Theraflu: Dangerous. All contain acetaminophen.
- Two different decongestants: Don’t stack Sudafed with Afrin for long, and never combine two oral decongestants.
- DXM + SSRIs or MAOIs: Serious serotonin syndrome risk.
- NSAIDs + blood thinners: Bleeding risk jumps.
I’ve seen a friend’s dad land in urgent care after pairing extra-strength Tylenol with regular Tylenol PM because the “PM” box didn’t look like a painkiller to him. Read labels every single time.
Table 2: Active Ingredient Dose Limits and Key Risks
| Active Ingredient | Max Daily Adult Dose | Key Risk at Overdose | Primary USA Source |
| Acetaminophen | 4,000 mg (3,000 mg if daily drinker) | Acute liver failure | FDA |
| Ibuprofen | 3,200 mg (OTC cap 1,200 mg) | GI bleeding, kidney injury | NIH MedlinePlus |
| Pseudoephedrine | 240 mg | Blood pressure spike, arrhythmia | FDA / DEA |
| Dextromethorphan | 120 mg | Serotonin syndrome, dissociation | NIH PubChem |
| Diphenhydramine | 300 mg | Anticholinergic delirium (elderly) | AAFP |
| Guaifenesin | 2,400 mg | Nausea, vomiting | NIH MedlinePlus |
Special Situations: Pregnancy, Kids, Seniors, Chronic Conditions
Standard advice doesn’t cover everyone. Here’s what shifts when you’re not a healthy 35-year-old.
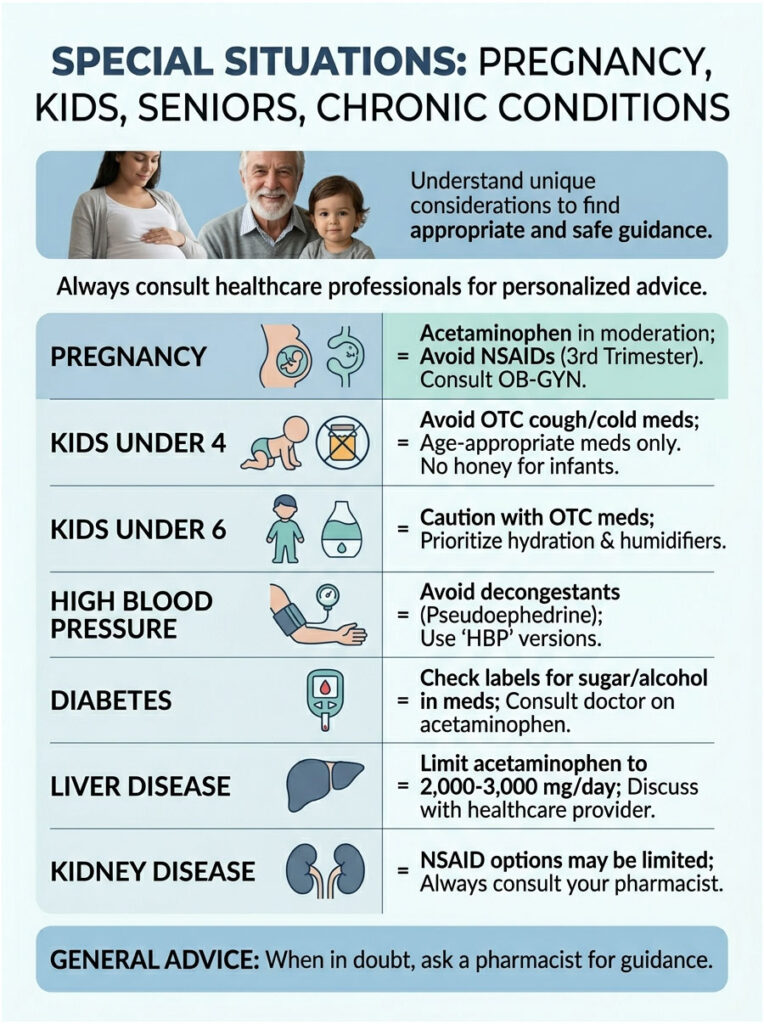
Pregnancy
Acetaminophen is the go-to pain reliever during pregnancy, used in moderation. NSAIDs are generally avoided, especially in the third trimester (risk to the fetal ductus arteriosus). Pseudoephedrine is usually avoided in the first trimester. Saline rinses, honey for cough, and rest are the safest tools. Always clear specifics with your OB-GYN.
Kids Under 4 (and Under 6)
The FDA does not recommend OTC cough and cold medicines for children under 4 and advises caution for ages 4 to 6. For infants and toddlers, stick to age-appropriate acetaminophen or ibuprofen, a cool-mist humidifier, nasal saline drops with a bulb syringe, and plenty of fluids. Never give honey to children under 12 months because of infant botulism risk.
Cold Medicine with High Blood Pressure
This is where I see the most dangerous mistakes. The American Heart Association warns that decongestants like pseudoephedrine can raise blood pressure and reduce the effectiveness of hypertension medication. Look for “HBP” versions of Coricidin and similar products, which skip the decongestant. Nasal saline rinses and steroid sprays are safer choices for congestion.
Diabetes, Liver, and Kidney Disease
Many liquid cold medicines contain sugar or alcohol; diabetics should check labels. Anyone with liver disease or regular alcohol use should cap acetaminophen at 2,000 to 3,000 mg daily and talk to a doctor first. Kidney disease narrows NSAID options. When in doubt, ask your pharmacist; they’re free and underused.
Home Remedies That Actually Work
Pills aren’t your only tool. These are the remedies with real research behind them.
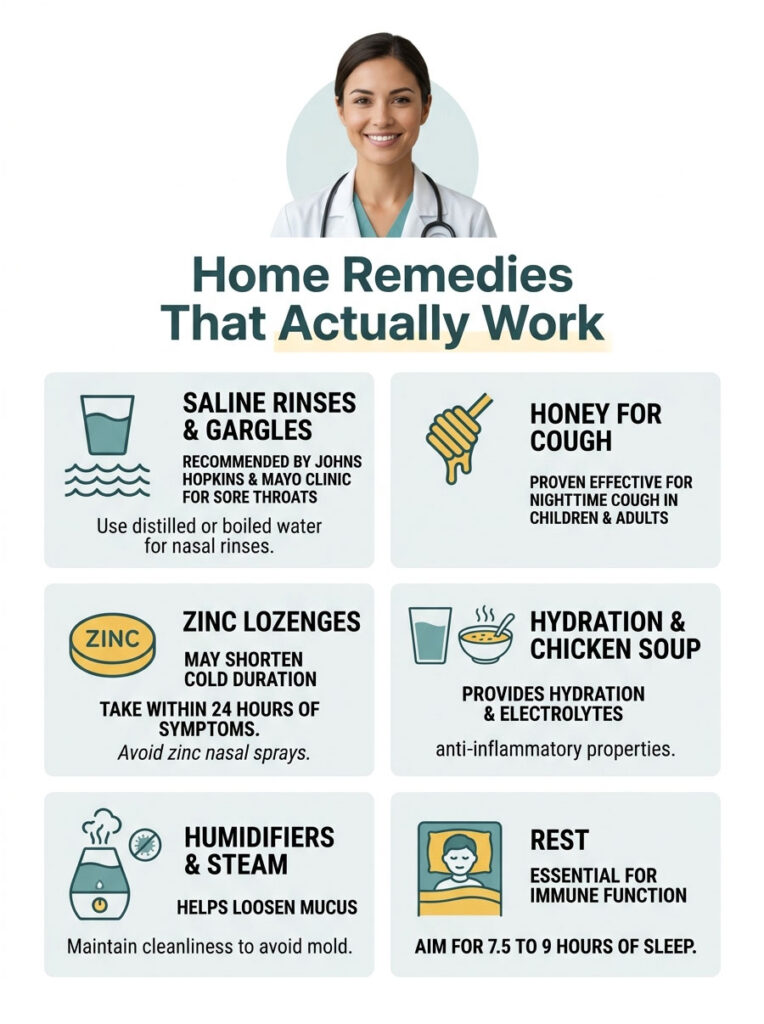
Saline rinses and gargles. Johns Hopkins and Mayo Clinic both back warm salt-water gargles for sore throat (about 1 teaspoon of salt per 8 oz of warm water). A daily saline nasal rinse with a neti pot or squeeze bottle clears mucus, reduces post-nasal drip, and makes steroid sprays work better. Use distilled or previously boiled water only.
Honey for cough. A 2018 Cochrane review found honey more effective than placebo for nighttime cough in kids over 1. Adults benefit too. One to two teaspoons straight, in warm tea, or stirred into water with lemon.
Zinc lozenges. Evidence is mixed but leaning positive if started within 24 hours of first symptoms. NIH notes that zinc gluconate or zinc acetate lozenges may shorten a cold’s duration by about a day. Skip zinc nasal sprays; the FDA warned they can cause permanent loss of smell.
Hydration and chicken soup. Not a joke. Chicken soup has modest anti-inflammatory evidence and hydrates while delivering electrolytes. Aim for 64 ounces of fluids daily, more if you’re feverish.
Humidifiers and steam. Warm humidified air loosens mucus. Clean the humidifier weekly to avoid mold.
Rest. Your immune system runs on sleep. Seven and a half to nine hours is the target. In my experience, skimping on sleep during a cold can double its duration.
What Doesn’t Work
- Antibiotics. Colds are viral. Antibiotics don’t help and contribute to resistance.
- High-dose vitamin C after symptoms start. Mayo Clinic notes little benefit once you’re already sick.
- Echinacea. Mixed studies, mostly negative.
- Zinc nasal sprays. FDA-flagged for anosmia (loss of smell).
Your 10-Day Cold Recovery Timeline
Colds follow a predictable arc. Knowing what’s coming keeps you calmer and helps you dose smarter.
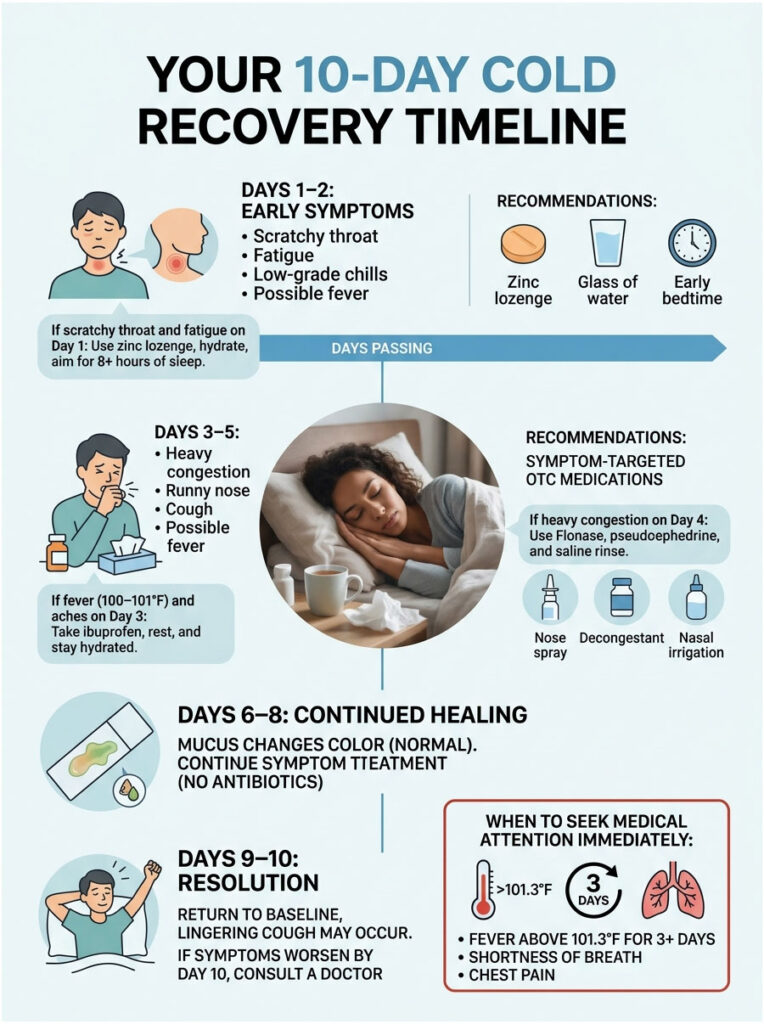
Day 1–2: Scratchy throat, fatigue, low-grade chills. This is when zinc lozenges, hydration, and an early bedtime do the most good.
Day 3–5: Peak symptoms. Congestion, runny nose, cough, sometimes fever. This is when symptom-targeted OTCs earn their keep.
Day 6–8: Mucus may turn yellow or green. That color alone doesn’t mean bacterial infection; it’s just immune cells doing their job. Keep treating symptoms.
Day 9–10: Most people are back to baseline. A lingering cough can persist another week or two (post-viral cough). If you’re not trending better by day 10, call a doctor.
Table 3: If-Then Action Guide by Day and Symptom
| Scenario | What’s Happening | Recommended Action |
| Day 1, scratchy throat + fatigue | Early viral replication | Zinc lozenge within 24 hrs, hydrate, sleep 8+ hrs |
| Day 3, fever 100–101°F + aches | Peak inflammatory response | Ibuprofen 400 mg every 6 hrs, fluids, rest |
| Day 4, heavy congestion, no sleep | Sinus swelling peak | Flonase + pseudoephedrine (daytime), saline rinse |
| Day 5, dry cough ruining sleep | Airway irritation | Delsym at bedtime, honey, humidifier |
| Day 7, green mucus but improving | Normal immune activity | Continue symptom care; no antibiotic needed |
| Day 10+, no improvement or worsening | Possible secondary infection | See a doctor; likely needs evaluation |
| Any day, fever above 101.3°F for 3+ days | Red flag | Call doctor same day |
| Any day, shortness of breath or chest pain | Emergency | Go to ER |
Red Flags: When to Stop Self-Treating
Most colds clear on their own. Some don’t. Know the signs that mean stop buying cough syrup and call a doctor.
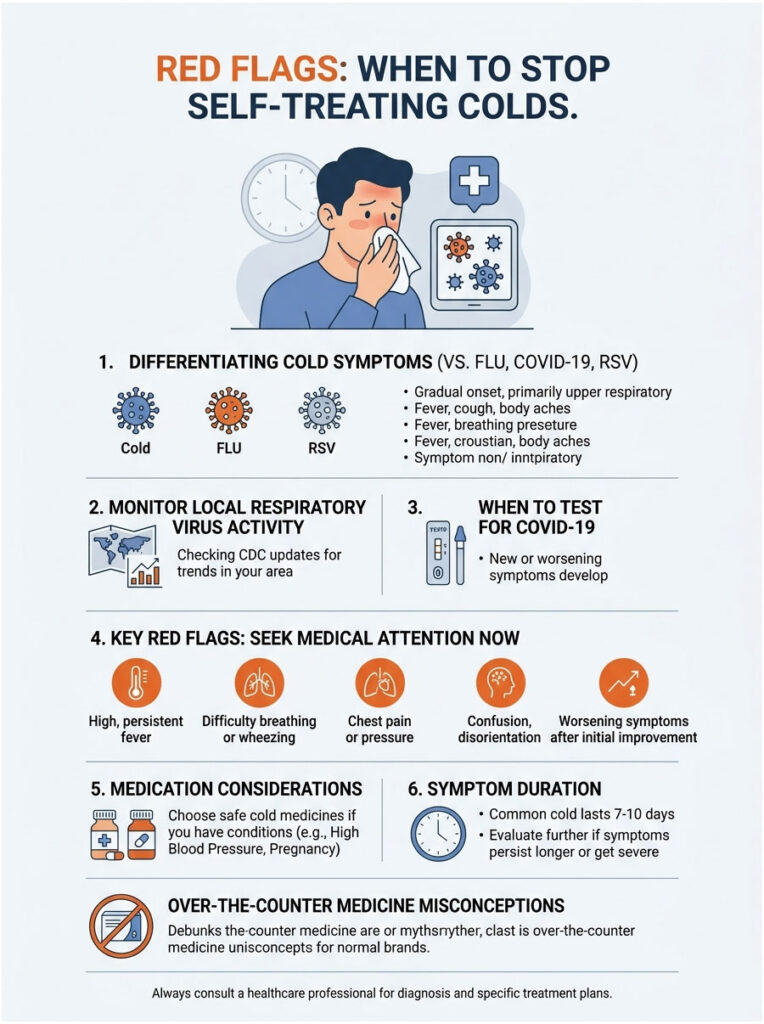
- Fever above 101.3°F (38.5°C) for 3 or more days
- Symptoms lasting longer than 10 days without clear improvement
- Shortness of breath, wheezing, or chest pain
- Severe sinus pain, especially one-sided
- Ear pain, muffled hearing, or drainage
- Coughing up blood or brown sputum
- Severe headache with stiff neck
- Symptoms that improve then suddenly worsen (classic bacterial superinfection pattern)
The CDC tracks respiratory virus activity weekly. If flu, RSV, or COVID is high in your area, test before assuming “just a cold.”
Cold vs. Flu vs. COVID-19 vs. RSV
| Feature | Common Cold | Flu | COVID-19 | RSV |
| Onset | Gradual (days) | Sudden (hours) | Variable | Gradual |
| Fever | Rare in adults | Common, high | Common | Moderate |
| Body aches | Mild | Severe | Moderate | Mild |
| Fatigue | Mild | Severe | Moderate to severe | Moderate |
| Cough | Mild to moderate | Moderate to severe | Common, dry | Wheezy, severe in infants |
| Loss of taste/smell | Rare | Rare | Possible | Rare |
If in doubt, test. At-home COVID tests are sold at every major US pharmacy, and many now run combination flu/COVID panels.
Frequently Asked Questions
What is the single best cold medicine on the market?
There isn’t one. The best cold medicine by symptom is whichever one matches your worst current complaint. For fever and aches, ibuprofen. For stuffy nose, pseudoephedrine or Flonase. For dry cough, Delsym. A combo pack is rarely your best option unless every symptom listed matches what you actually have.
Can I take Mucinex and Sudafed at the same time?
Yes. They target different problems (Mucinex thins mucus, Sudafed reduces nasal swelling) and have no overlapping active ingredient. Double-check that neither product is a combo formula already containing both, and watch pseudoephedrine if you have high blood pressure, since it can cause spikes.
How long does a cold actually last?
Most adult colds resolve in 7 to 10 days, per the CDC. Peak symptoms hit on days 3 to 5. A lingering dry cough can last 2 to 3 additional weeks (post-viral cough). If you’re not improving by day 10, it’s time to call a doctor for an evaluation.
What cold medicine is safe with high blood pressure?
Avoid oral decongestants like pseudoephedrine and phenylephrine, which can raise blood pressure. Safer picks include saline nasal rinses, Flonase or Nasacort nasal sprays, Claritin or Zyrtec for runny nose, and Tylenol or Mucinex for other symptoms. Look for “HBP” labeled cold products like Coricidin HBP.
Is NyQuil safe to take every night?
Short-term use (3 to 5 nights during a cold) is generally fine for healthy adults. Taking NyQuil nightly long-term isn’t advisable because of its acetaminophen content, alcohol in some versions, and doxylamine, which has anticholinergic effects linked to cognitive issues in older adults over time.
Does zinc really shorten a cold?
Possibly, if you start within 24 hours of symptoms. NIH research shows zinc gluconate or zinc acetate lozenges may shorten duration by about a day. Higher doses may cause nausea. Skip zinc nasal sprays because of anosmia risk flagged by the FDA.
Can I take Tylenol and ibuprofen together?
Yes. They work by different mechanisms and can be taken simultaneously or alternated for stubborn fever or pain. Stay under the max dose of each: 4,000 mg acetaminophen and 1,200 mg ibuprofen per day for OTC use. Avoid this combo if you have kidney, liver, or stomach issues.
What’s the strongest OTC decongestant now that phenylephrine is out?
Pseudoephedrine (real Sudafed) is the strongest oral decongestant on shelves, sold behind the pharmacy counter with ID required. For spray options, oxymetazoline (Afrin) works fast but can’t be used more than 3 consecutive days. Steroid sprays like Flonase take longer but are safer for long use.
What cold medicine can I take while pregnant?
Acetaminophen is usually the first choice for pain and fever. Saline nasal sprays, honey for cough, and rest are safe. Avoid ibuprofen, aspirin, and pseudoephedrine, especially in the first and third trimesters. Always confirm specific brands and doses with your OB-GYN.
At what point should I go to urgent care for a cold?
Go if you have a fever over 101.3°F for 3+ days, symptoms worsening after day 7, shortness of breath, chest pain, coughing blood or brown mucus, severe sinus or ear pain, or symptoms lasting more than 10 days. Go sooner if you’re elderly, pregnant, immunocompromised, or have chronic heart or lung disease.
Why does my cold always get worse at night?
Lying flat lets mucus pool in your throat and sinuses, gravity no longer helps drainage, and cortisol (your natural anti-inflammatory) drops at night. Elevate your head with an extra pillow, run a humidifier, use saline spray, and consider nighttime formulas with antihistamines if sleep is the issue.
Can I give my child cold medicine safely?
Children under 4 should not get OTC cough and cold medicine, per FDA guidance. Ages 4 to 6 need pediatrician approval. Use weight-based children’s acetaminophen or ibuprofen (ages 6 months+) for fever, a cool-mist humidifier, saline drops, and fluids. Honey works for cough in kids 1 and older; never under age 1.
| Disclaimer This article is for educational purposes only and does not replace medical advice from a licensed healthcare provider. Always read product labels, consult your pharmacist about drug interactions, and call your doctor or 911 for urgent symptoms. Medication doses listed are general adult guidance; your specific situation may require different amounts. |
References
- Centers for Disease Control and Prevention: About Common Cold
- CDC: Respiratory Virus Activity Levels
- Food and Drug Administration: Acetaminophen Information
- FDA: When to Give Kids Medicine for Coughs and Colds
- Mayo Clinic: Cold Remedies, What Works, What Doesn’t
- Johns Hopkins Medicine: The Do’s and Don’ts of Easing Cold Symptoms
- American Heart Association: OTC Medications and High Blood Pressure
- American Academy of Family Physicians
- NIH Office of Dietary Supplements: Zinc Fact Sheet
- NIH MedlinePlus: Cold and Cough Medicines
- UCLA Health: A Guide to Cold Medicines





