
You picked up your CBC printout from the lab, ran a finger down the column, and stopped on the line marked RDW. Next to it sits a small “H,” sometimes circled in red, sometimes flagged in bold by your patient portal. Your hemoglobin might look fine. Your white cells, fine. But that one number is high, and your search history is suddenly full of frantic 11 p.m. questions. Take a breath. A high RDW blood test is rarely an emergency, but it almost always deserves a follow-up. Here is what it means, what your US doctor will likely do next, and how to act on it sensibly.
Table of Contents
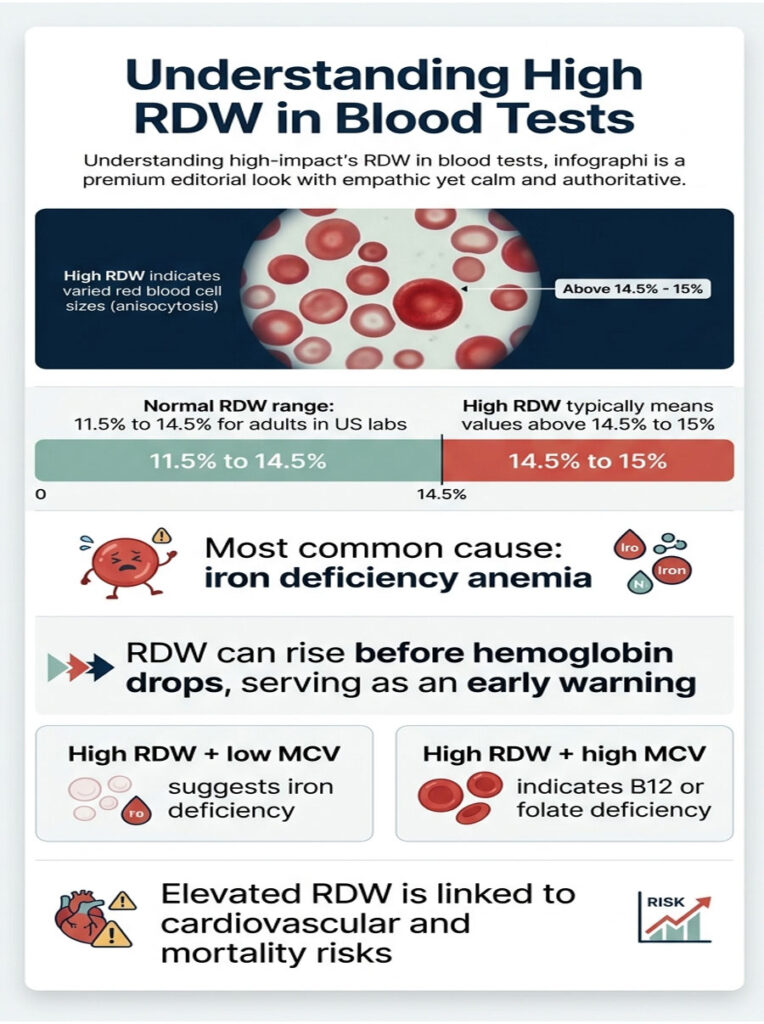
Quick Answer: A high RDW blood test means your red blood cells vary in size more than normal, a state called anisocytosis. The most common cause is iron deficiency anemia, followed by vitamin B12 or folate deficiency, mixed anemia, chronic disease, recent blood loss, and rarely bone marrow disorders. Doctors interpret RDW alongside hemoglobin and MCV, then order targeted follow-up labs. Most cases improve in 4 to 8 weeks once the underlying cause is treated.
At a Glance
• Normal adult RDW range in US labs is roughly 11.5% to 14.5%
• “High RDW” usually means a value above 14.5% to 15%, depending on the lab
• Iron deficiency is the single most common cause in American adults
• RDW often rises before hemoglobin drops, making it an early warning
• High RDW + low MCV typically points to iron deficiency
• High RDW + high MCV typically points to B12 or folate deficiency
• Persistently elevated RDW is linked to cardiovascular and mortality risk in research literature
• Most causes are treatable; targeted lab work-up is the next step
What Is the RDW Blood Test?
RDW stands for Red Cell Distribution Width. It is a routine measurement on every standard complete blood count (CBC) ordered through US labs like LabCorp and Quest Diagnostics.
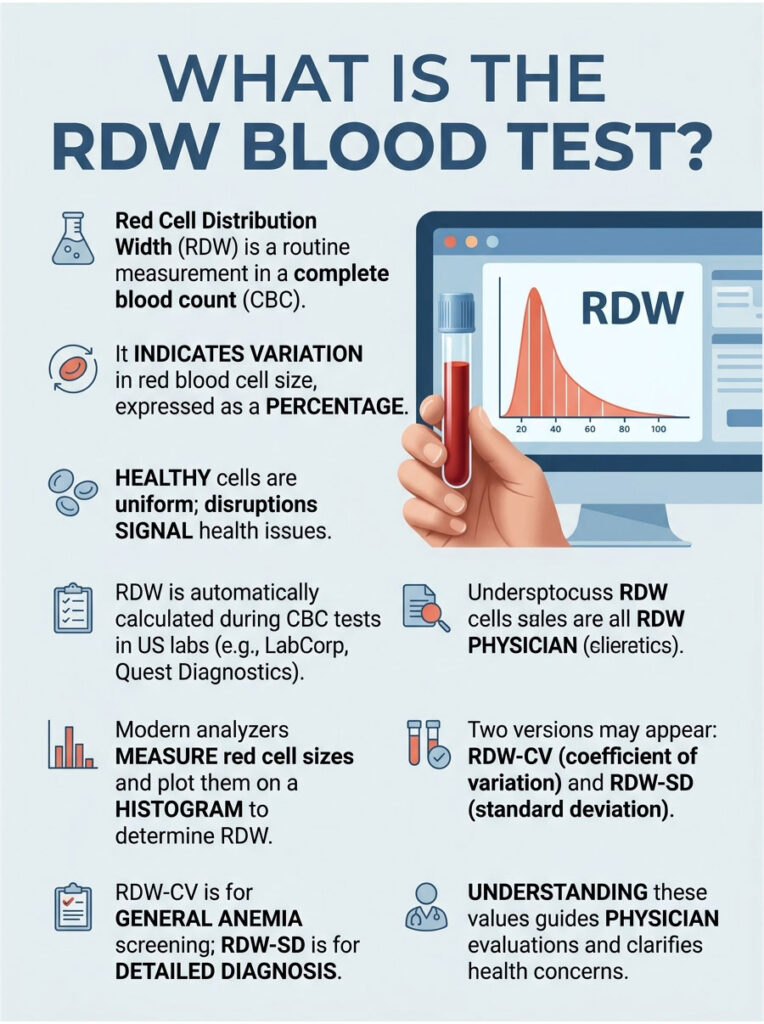
The test reports how much your red blood cells differ from each other in size, expressed as a percentage. Healthy red blood cells are remarkably uniform in volume, like coins from the same mint.
When something disrupts that uniformity (low iron, low B12, recent bleeding, chronic disease), newer cells get produced at different sizes. RDW captures that scatter on a single line of your report.
Our medical reviewers at HealthCareOnTime note that RDW is one of the most under-explained values in patient lab summaries. Most online sources skip the fact that there are actually two versions of this number on US lab reports, and the difference matters more than patients realize.
How RDW Is Measured in US Labs
Modern hematology analyzers run your blood through a flow chamber, measure each red cell electronically, and plot the sizes on a histogram. RDW is the statistical width of that histogram.
A narrow histogram means uniform cells, giving a low RDW. A wide histogram means variable cells, giving a high RDW. Per MedlinePlus (NIH), RDW is automatically calculated on every CBC, even if your doctor never asked for it specifically. Almost every American adult has at least one RDW value sitting in their patient portal right now.
RDW-CV vs RDW-SD: Which One Is on Your Report?
This is the detail almost every Page 1 article skips. US lab reports may show RDW-CV (coefficient of variation, expressed as %) or RDW-SD (standard deviation, expressed in femtoliters, fL).
RDW-CV is the more common reading on consumer reports, with a typical normal range of 11.5% to 14.5%. RDW-SD is the absolute spread of cell sizes, with a normal range of roughly 39 to 46 fL.
Patients booking lab work through HealthCareOnTime often ask why their two values disagree. The answer: they measure related but distinct things. Your physician will look at the one most relevant to your case, usually RDW-CV for general anemia screening and RDW-SD for finer differential diagnosis.
What Is the Normal RDW Range? (USA Reference Chart)
Normal RDW ranges shift slightly by lab, by age, and by life stage. The Cleveland Clinic lists 12% to 15% as a typical normal band. LabCorp and Quest Diagnostics commonly use 11.5% to 14.5%.
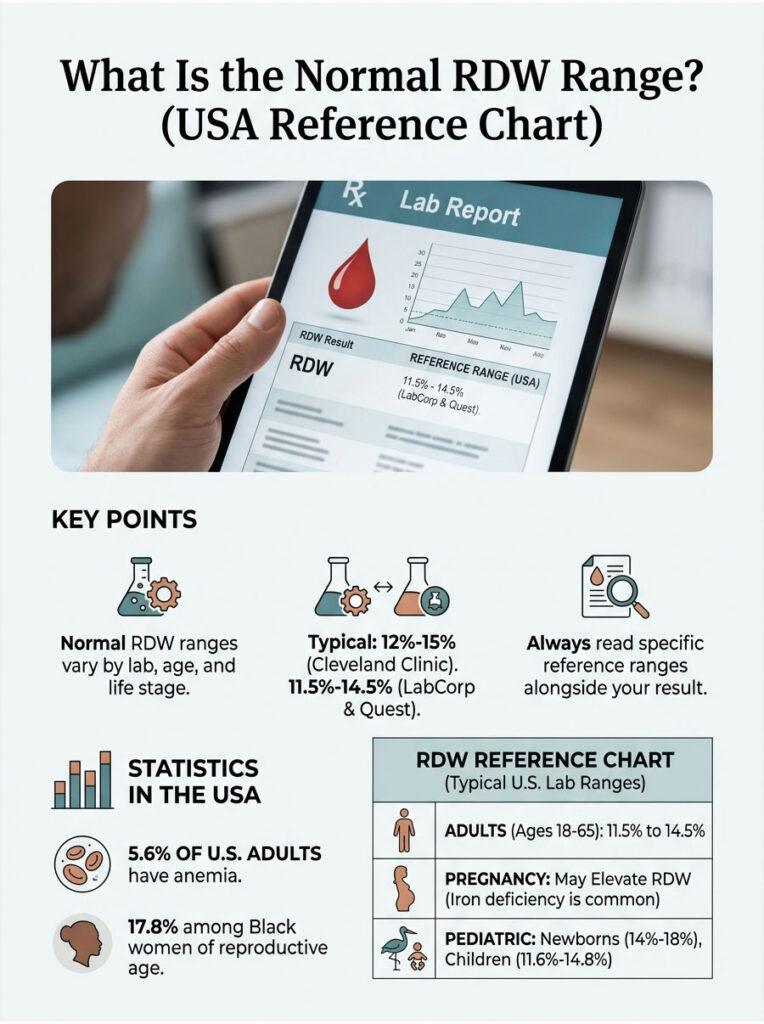
The takeaway is straightforward: read your specific lab’s reference range printed beside your value. According to CDC NHANES surveillance data, roughly 5.6% of US adults meet the criteria for anemia, with rates climbing to about 17.8% among Black women of reproductive age. Many of these cases first surface as a high RDW before hemoglobin falls outside normal limits.
Adult RDW Range
For most American adults aged 18 to 65, an RDW between 11.5% and 14.5% is considered normal. Our medical content team verifies these ranges against current LabCorp and Quest Diagnostics reference tables, the two largest US reference labs.
Pediatric RDW Range
Children typically run slightly higher than adults, especially under age 2. Newborns can sit between 14% and 18% in their first weeks of life and still be perfectly healthy as their fetal hemoglobin transitions to adult hemoglobin. Pediatricians read these values in age-specific context, never against adult thresholds.
RDW During Pregnancy
Pregnancy stresses iron stores. The American College of Obstetricians and Gynecologists (ACOG) flags iron deficiency in roughly half of US pregnancies by the third trimester.
A high RDW in pregnancy is common and often reflects iron-deficient erythropoiesis even before overt anemia develops. Routine screening of hemoglobin and ferritin in each trimester catches most cases early.
Table 2: USA RDW Reference Ranges by Demographic
| Demographic Group | Typical RDW-CV Range | Typical RDW-SD Range | Notes | Source |
| Adult men (18-65) | 11.5% to 14.5% | 39-46 fL | Stable across age | LabCorp |
| Adult women (18-50) | 11.5% to 14.5% | 39-46 fL | Higher anemia risk during menses | Quest Diagnostics |
| Pregnant women | 12.0% to 15.5% | 40-48 fL | Rises mildly each trimester | ACOG |
| Children (2-12) | 11.6% to 14.8% | 38-46 fL | Slightly wider in toddlers | Cleveland Clinic |
| Adults 65+ | 12.0% to 15.5% | 40-48 fL | Anemia of aging is common | NIH MedlinePlus |
What Does a High RDW Mean?
A high RDW means your blood holds a mix of red cells in noticeably different sizes. The medical word is anisocytosis, from Greek roots meaning “unequal cells.” It is a finding, not a diagnosis.
Your bone marrow produces about 2 million new red cells every second. When the supply of building blocks is steady, those cells come out uniform. When iron, B12, folate, or oxygen delivery is disrupted, the marrow produces cells of different sizes, and RDW climbs.
Across cases reviewed by our diagnostic network, RDW frequently rises before hemoglobin falls below the normal cutoff. That makes it one of the earliest signals of nutritional or systemic trouble, sometimes weeks before any symptom appears.
The American Society of Hematology (ASH) recognizes this early-warning property, which is why physicians take a high RDW seriously even when other CBC values look fine. A 2018 review in BioMed Research International on RDW in clinical settings catalogues over 30 conditions associated with elevated RDW values, ranging from common anemias to severe systemic disease.
The point: a high RDW asks a question, and the question deserves an answer.
9 Causes of High RDW Blood Test
The most common American patterns, ordered from frequent to rare:
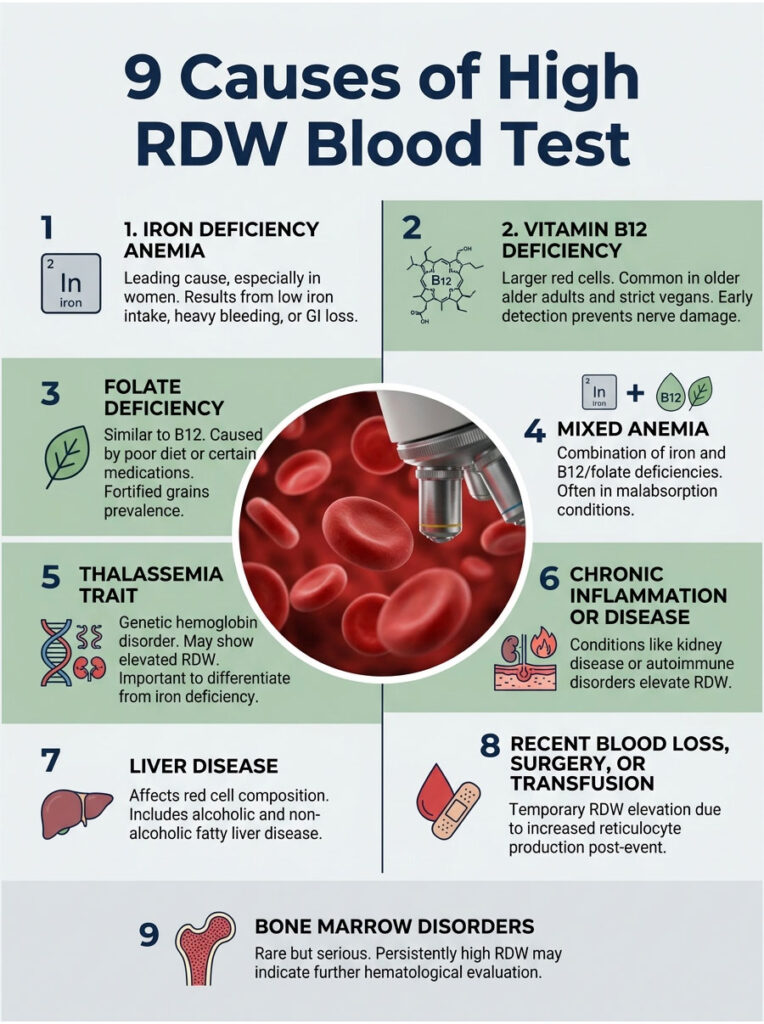
1. Iron Deficiency Anemia (Most Common in US Women)
Iron deficiency leads the list across every US age group. Heavy menstrual bleeding, low dietary iron, pregnancy, and gastrointestinal blood loss are the usual drivers.
As iron runs out, the marrow turns out smaller cells, while older normal-sized cells are still circulating. The size scatter widens, and RDW rises early, often before hemoglobin drops.
2. Vitamin B12 Deficiency
B12 deficiency produces larger-than-normal red cells. It is common in older Americans, strict vegans, people on long-term metformin or proton-pump inhibitors, and those with pernicious anemia (an autoimmune cause).
Symptoms can include numbness in the hands or feet, balance trouble, glossitis (sore tongue), and brain fog. Untreated B12 deficiency can cause permanent nerve damage, which is why early detection matters.
3. Folate Deficiency
Folate (vitamin B9) deficiency mimics B12 deficiency on labs, producing macrocytic red cells. Causes include poor diet, pregnancy, alcohol misuse, and certain medications like methotrexate.
The CDC’s mandatory folate fortification of US grain products since 1998 has cut these cases significantly, but they still appear regularly, especially in alcohol use disorder and post-bariatric surgery patients.
4. Mixed Anemia
When iron deficiency and B12 or folate deficiency exist together (small cells and large cells in the same bloodstream), RDW spikes high, sometimes well above 17%.
This is common in malabsorption syndromes, post-bariatric surgery patients, and people with celiac disease. Mixed anemia is one of the trickiest patterns to spot from the CBC alone, which is why iron studies and B12/folate panels are typically ordered together.
5. Thalassemia Trait
Thalassemia is an inherited condition affecting hemoglobin production. It is more common in Americans of Mediterranean, South Asian, Southeast Asian, and African ancestry.
RDW is sometimes elevated in thalassemia, though classic thalassemia trait often shows a normal RDW with low MCV. That distinction is a useful clue for telling it apart from iron deficiency and avoiding unnecessary iron supplementation.
6. Chronic Inflammation or Disease
Long-running illness disrupts red cell production. CDC data shows about 1 in 7 US adults has chronic kidney disease, and many of them carry an elevated RDW.
Other examples include rheumatoid arthritis, lupus, inflammatory bowel disease, and chronic infections. Anemia of chronic disease is a recognized US clinical category with its own treatment pathway.
7. Liver Disease
Liver dysfunction changes red cell membrane composition and raises RDW. Common American causes include alcoholic liver disease, viral hepatitis, and non-alcoholic fatty liver disease (NAFLD).
NAFLD now affects roughly 25% of US adults per NIH NIDDK data, making it a frequent silent contributor to abnormal CBC findings.
8. Recent Blood Loss, Surgery, or Transfusion
After surgery, a GI bleed, trauma, or even blood donation, the bone marrow ramps up reticulocyte production. These young cells are larger, mixing with older normal cells and pushing RDW up temporarily.
The reticulocyte count, which our medical reviewers consistently flag as the most underused follow-up test, helps confirm this pattern within minutes of being run.
9. Bone Marrow Disorders (Rare but Serious)
Conditions like myelodysplastic syndromes (MDS) and aplastic anemia produce abnormally sized cells. These are uncommon, but a persistently very high RDW (above 18%) combined with other CBC abnormalities warrants hematology referral.
Most US hematologists will rule these out using peripheral smear, reticulocyte count, and, if indicated, bone marrow biopsy.
Decoding RDW + MCV Combinations (The Diagnostic Cheat Sheet)
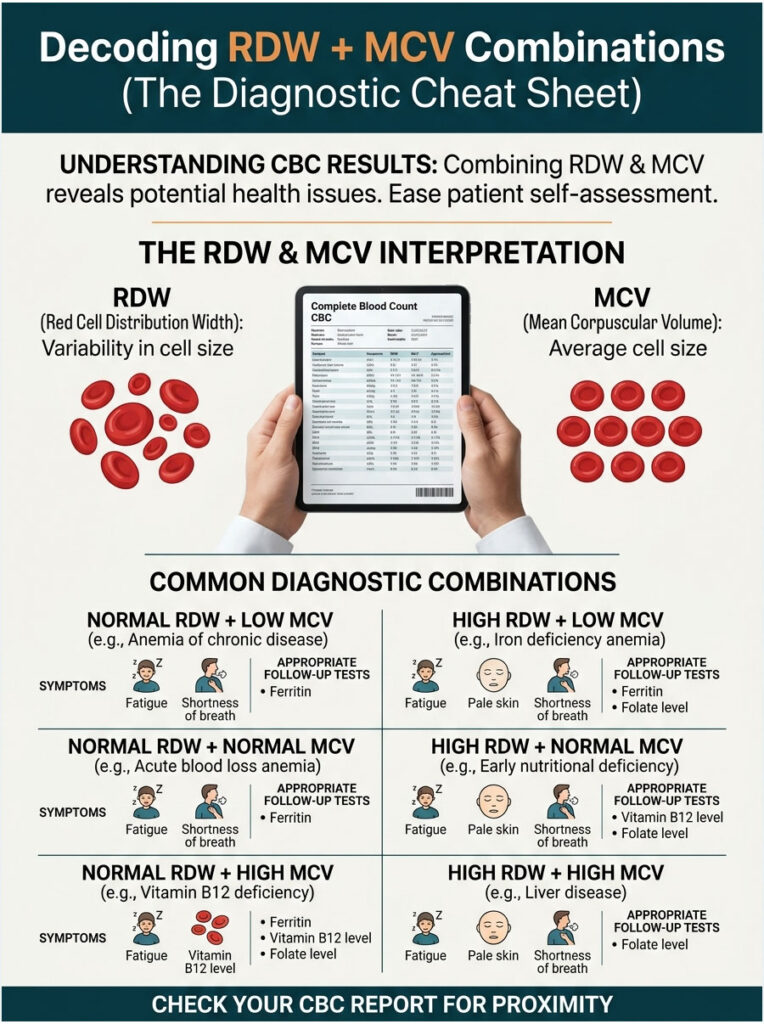
This is the single most useful frame for interpreting your CBC at home, and it is missing from almost every Page 1 result on Google. RDW alone tells you cells vary in size. MCV tells you what the average size is. Combine them and the likely cause becomes obvious.
In tests booked through HealthCareOnTime, this combination chart is the most-saved patient resource by a wide margin. It turns four CBC numbers into a clear next step without a medical degree.
Table 1: RDW + MCV Diagnostic Combinations
| RDW | MCV | Likely Cause | Common Symptoms | Recommended Follow-Up Tests |
| High | Low | Iron deficiency anemia | Fatigue, pale skin, brittle nails, cold hands | Ferritin, serum iron, TIBC, transferrin saturation |
| High | High | B12 or folate deficiency | Tingling, glossitis, memory issues, weakness | Serum B12, folate, methylmalonic acid, homocysteine |
| High | Normal | Early or mixed anemia | Subtle fatigue, often pre-symptomatic | Reticulocyte count, ferritin, B12, folate |
| Normal | Low | Thalassemia trait | Often asymptomatic | Hemoglobin electrophoresis, ferritin |
| Normal | High | Liver disease, alcohol use, hypothyroidism | Variable | Liver panel, TSH, B12 |
| Normal | Normal | No anemia indicated | None typically | Routine monitoring |
If your RDW is high and you do not know your MCV, scroll back up your CBC printout. The two values usually sit two lines apart on standard US lab reports.
High RDW but Hemoglobin Normal: What It Really Means
This is one of the most-searched anxiety queries in the entire RDW category, and it deserves a straight answer. A high RDW with normal hemoglobin is not an emergency, but it is not nothing either.
It usually means one of three things. First, you may be in the early stage of a developing anemia. Iron, B12, or folate stores are running low; the marrow is starting to produce uneven cells, but hemoglobin has not yet dropped below the cutoff. Catching it now avoids fatigue later.
Second, you may be recovering from a recent stressor, such as blood loss, surgery, or a recent transfusion. Younger reticulocytes are larger and mix with mature cells, lifting RDW for a few weeks.
Third, low-grade chronic inflammation or early kidney or liver dysfunction can quietly raise RDW without dropping hemoglobin yet. Patients booking CBC tests with HealthCareOnTime often ask whether to repeat the test before panicking. In most cases, our medical team recommends a recheck in 4 to 8 weeks plus targeted iron studies, rather than waiting passively.
When Is a High RDW Dangerous?
Most high RDW results are mild and not urgent. The value alone does not determine danger; the combination of RDW with hemoglobin, symptoms, and underlying cause does.
Approximate clinical thresholds American physicians use to gauge urgency:
- 14.6% to 16.0%: Mildly elevated. Often early nutritional deficiency. Routine follow-up.
- 16.1% to 18.0%: Significantly elevated. Established anemia or chronic disease likely. Targeted work-up needed.
- Above 18.0%: Markedly elevated. Mixed anemia, severe deficiency, or possible bone marrow disorder. Hematology referral typically warranted.
Call 911 or go to the ER if a high RDW result appears with severe shortness of breath, chest pain, fainting, rapid heart rate, black or bloody stools, or vomiting blood. These point to severe anemia or acute internal bleeding, which need immediate care, not a clinic appointment.
For everyone else, a primary care visit within 1 to 2 weeks is the right pace. Across patients we serve, the largest mistake is ignoring the result for months because nothing feels acutely wrong, only to walk into a far harder problem later.
RDW as a Prognostic Marker (What Top 3 Articles Missed)
Beyond anemia, RDW has become one of the most studied prognostic markers in modern medicine. Almost no consumer health article on Page 1 covers this, even though hundreds of peer-reviewed papers have been published on it.
A landmark study from the Intermountain Medical Center Heart Institute found that elevated RDW correlates with worse outcomes in patients with heart failure, including higher rates of hospitalization and mortality.
A 2019 review in the Journal of Translational Medicine synthesized evidence linking RDW with chronic inflammation and oxidative stress markers, supporting its use as a general “stress signal” beyond hematology.
RDW has been studied as a prognostic marker in:
- Acute and chronic heart failure
- Coronary artery disease and post-MI outcomes
- Stroke severity and recovery
- Several cancers, including colorectal, lung, and pancreatic
- COVID-19 severity, with multiple 2020 to 2022 studies linking elevated RDW on admission with higher mortality risk
- Sepsis outcomes in ICU patients
The takeaway is not that high RDW causes these conditions. It does not. It is a downstream marker of systemic stress on the body’s red cell production.
Our clinical content team frames it this way: RDW is the canary, not the coal mine. When the canary signals, you investigate.
How Doctors Diagnose the Cause (US Workup Process)
Once a high RDW is confirmed, sometimes after a recheck CBC, American physicians follow a stepwise lab pathway. The aim is to narrow nine possibilities to one or two without ordering every test in the book.
Tests Your US Doctor Will Order Next
The standard follow-up panel typically includes:
- Ferritin (the single best iron storage marker)
- Serum iron, TIBC, transferrin saturation (iron transport markers)
- Vitamin B12 and methylmalonic acid (if low-normal B12)
- Folate
- Reticulocyte count (to assess marrow response)
- Comprehensive metabolic panel (kidney and liver function)
- TSH (thyroid screening)
- Hemoglobin electrophoresis (if hereditary cause suspected)
- Peripheral blood smear (if MDS or unusual cells suspected)
Approximate US Lab Costs
Out-of-pocket retail pricing through LabCorp or Quest Diagnostics typically runs:
- Ferritin: $40 to $90
- Vitamin B12: $25 to $60
- Folate: $20 to $50
- Reticulocyte count: $15 to $40
- Comprehensive iron panel: $60 to $120
Most US health plans cover these tests when ordered for a flagged CBC. HSA and FSA dollars also apply. In labs partnered with HealthCareOnTime, packaged anemia work-ups often come in below the sum of individual tests.
When You’ll See a Hematologist
Primary care handles roughly 90% of high RDW cases in the United States. Referral to hematology is typical if:
- RDW is persistently above 18%
- Multiple CBC abnormalities cluster together (low platelets, low white cells, plus high RDW)
- There is an unexplained drop in hemoglobin not responsive to supplementation
- MDS, aplastic anemia, or another marrow disorder is on the differential
- The patient has a personal or family history of hematologic malignancy
Treatment by Cause (What Actually Works)
Treating high RDW means treating the underlying cause. There is no medication that “lowers RDW” directly. Once the cause is corrected, RDW normalizes on its own as the bone marrow produces a fresh, uniform population of red cells.
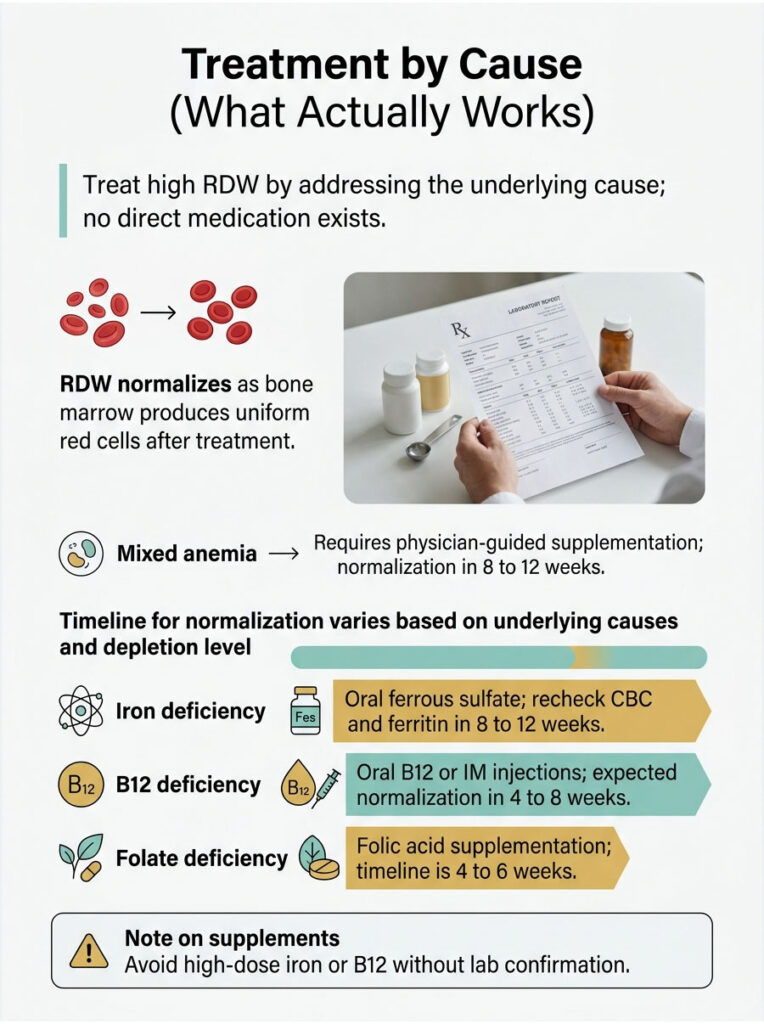
This typically takes 4 to 8 weeks, sometimes up to 3 months for iron deficiency. The pace depends entirely on the cause and how depleted your stores were at baseline.
Table 3: Treatment Decision Matrix by Cause
| Scenario | Recommended Action | Expected Timeline to Normalize RDW |
| Iron deficiency confirmed (low ferritin) | Oral ferrous sulfate 65 mg elemental iron daily or every other day; recheck CBC and ferritin in 8 to 12 weeks | 8 to 12 weeks |
| B12 deficiency confirmed | Oral B12 1,000 to 2,000 mcg daily, or IM injections if absorption issue | 4 to 8 weeks |
| Folate deficiency confirmed | Folic acid 1 mg daily orally; address underlying cause (diet, alcohol, methotrexate) | 4 to 6 weeks |
| Mixed anemia (iron + B12) | Sequential or combined supplementation under physician guidance; rule out malabsorption | 8 to 12 weeks |
| Chronic kidney disease anemia | Manage CKD; erythropoiesis-stimulating agents may apply per nephrology | Ongoing |
| Recent blood loss, post-surgical | Iron replenishment, recheck in 6 to 8 weeks | 4 to 8 weeks |
| Suspected MDS or marrow disorder | Hematology referral, bone marrow biopsy if indicated | Variable |
A note on supplements: never start high-dose iron, B12, or folate without confirmed lab results. Iron overload is real, especially in men and post-menopausal women.
Folate alone can mask undiagnosed B12 deficiency, allowing nerve damage to progress silently. Our medical reviewers see this pattern repeatedly in patients who self-prescribed before testing.
How to Lower RDW Naturally (US Diet & Lifestyle)
If the cause is nutritional, food can do most of the work. Diet alone will not fix RDW driven by chronic disease, blood loss, or marrow disorders. But for the most common American causes, what you eat matters.
Iron-rich foods (heme iron, best absorbed):
- Lean beef sirloin: about 2.7 mg per 3 oz
- Beef liver: about 5 mg per 3 oz
- Sardines (canned in oil): about 2.4 mg per 3 oz
- Chicken thigh, dark meat: about 1.3 mg per 3 oz
- Oysters: about 8 mg per 3 oz
Plant iron sources (non-heme; pair with vitamin C):
- Cooked spinach: about 6.4 mg per cup
- Lentils: about 6.6 mg per cup cooked
- Fortified breakfast cereals (US standard): 8 to 18 mg per serving
- White beans: about 8 mg per cup cooked
- Pumpkin seeds: about 2.5 mg per ounce
Vitamin B12 sources:
- Beef liver, salmon, tuna, dairy, eggs
- Fortified nutritional yeast and B12-fortified plant milks for vegans
- B12 sublingual tablets, often used by older adults with absorption issues
Folate sources:
- Dark leafy greens (spinach, romaine, kale)
- Asparagus, Brussels sprouts, broccoli
- Lentils, black beans, chickpeas
- Citrus fruits, avocado
- Fortified US grain products (mandated since 1998)
Hydration helps too. Mild chronic dehydration can subtly distort CBC indices in ways that are hard to predict. Adults should aim for 64 to 96 oz of water daily, more in hot climates or during exercise.
Patients commonly ask us about iron supplements vs food alone. For confirmed iron deficiency anemia, food alone usually cannot rebuild stores fast enough; supplementation under medical guidance is standard US practice. For mild RDW elevation without anemia, dietary changes plus a recheck often suffice.
Frequently Asked Questions
What level of RDW is dangerous?
There is no universal “dangerous” cutoff, but most US clinicians consider RDW above 18% markedly elevated and worth urgent follow-up, especially if hemoglobin is also low. Values between 14.6% and 16% are mildly elevated and usually managed in primary care with targeted lab work and a recheck CBC.
Is an RDW of 15.5% high?
A reading of 15.5% sits just above the typical US lab upper limit of 14.5%. It counts as mildly elevated, often signaling early iron, B12, or folate deficiency before hemoglobin drops. Our medical team recommends iron studies and a CBC recheck in 4 to 8 weeks rather than ignoring the result.
What is the most common cause of high RDW in adults?
Iron deficiency anemia leads in US adults, especially among women of reproductive age, vegetarians, and people with heavy menstrual bleeding or chronic GI blood loss. CDC NHANES data places anemia prevalence near 5.6% of US adults, with iron deficiency accounting for the majority of those cases.
Can dehydration cause a high RDW reading?
Mild dehydration usually does not change RDW meaningfully. Severe dehydration can subtly distort CBC indices, but RDW reflects red cell size variation, which dehydration does not directly alter. If your RDW is high, hydration is unlikely to be the explanation, and targeted lab follow-up is the better path.
How long does it take for RDW to return to normal?
Once the underlying cause is treated, RDW typically normalizes in 4 to 8 weeks for B12 or folate deficiency, and 8 to 12 weeks for iron deficiency. Mixed deficiencies take longer, often 12 weeks or more. Chronic conditions like CKD or marrow disorders may keep RDW elevated long-term.
What is the difference between RDW-CV and RDW-SD on my report?
RDW-CV is a percentage measuring how much red cell sizes vary relative to the average; normal range is roughly 11.5% to 14.5%. RDW-SD is the absolute spread in femtoliters; normal is about 39 to 46 fL. Most US patient portals show RDW-CV by default, though both can appear.
Should I worry if my RDW is high but my hemoglobin is normal?
This pattern often means an early-stage deficiency, recent recovery from blood loss, or low-grade chronic inflammation. It is not an emergency, but it is also not nothing. Our medical reviewers recommend ferritin, B12, folate testing, and a CBC recheck in 4 to 8 weeks to identify the cause early.
Can high RDW indicate cancer?
Persistently elevated RDW has been studied as a prognostic marker in cancers like colorectal, lung, and pancreatic, but a high RDW alone does not diagnose cancer. It is a non-specific marker of physiologic stress. Cancer work-up is only triggered when other findings (weight loss, GI bleeding, abnormal imaging, family history) raise suspicion.
Does pregnancy raise RDW levels?
Yes, mildly. Iron demand spikes in the second and third trimesters, and many pregnant Americans develop iron-deficient erythropoiesis even without overt anemia. ACOG recommends screening hemoglobin and ferritin during pregnancy. A slightly elevated RDW combined with low ferritin usually responds well to oral iron supplementation.
Can stress or lack of sleep affect RDW?
Acute psychological stress and short-term sleep loss generally do not change RDW directly. Chronic stress that leads to chronic inflammation, poor diet, or worsening underlying disease can indirectly raise RDW over time. The fix is addressing the upstream driver, not chasing RDW with lifestyle tweaks alone.
What doctor should I see for a high RDW result?
Start with your primary care physician or internist. They handle the majority of high RDW work-ups in the United States. Referral to hematology is typical only when RDW is persistently above 18%, multiple CBC values are abnormal, or initial labs do not identify a cause. OB-GYN handles pregnancy-related cases.
Can children have a high RDW?
Yes. Mild RDW elevation in toddlers is common during rapid growth phases and is most often nutritional. Pediatricians evaluate using age-specific reference ranges. Severe or persistent elevation in a child warrants pediatric hematology evaluation, especially if hemoglobin is also low or growth is affected.
Medical Disclaimer: This article is for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. The content reflects general guidance reviewed by the HealthCareOnTime medical content team and current US clinical references as of publication. Always speak with your physician about your specific lab results, symptoms, and treatment options. Never start, stop, or change supplements or medications without medical guidance.
References
- Centers for Disease Control and Prevention (CDC), National Health and Nutrition Examination Survey (NHANES): https://www.cdc.gov/nchs/nhanes/index.htm
- MedlinePlus, US National Library of Medicine, NIH, Red Cell Distribution Width (RDW): https://medlineplus.gov/lab-tests/rdw-red-cell-distribution-width/
- Cleveland Clinic, RDW Blood Test: https://my.clevelandclinic.org/health/diagnostics/22980-rdw-blood-test
- American Society of Hematology (ASH): https://www.hematology.org/
- American College of Obstetricians and Gynecologists (ACOG): https://www.acog.org/
- Mayo Clinic, Anemia overview: https://www.mayoclinic.org/diseases-conditions/anemia
- NIH National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK): https://www.niddk.nih.gov/
- Salvagno GL et al., “Red cell distribution width: A simple parameter with multiple clinical applications,” Critical Reviews in Clinical Laboratory Sciences
- Intermountain Medical Center Heart Institute, RDW research summaries: https://intermountainhealthcare.org/
- Wen Y et al., “Red Blood Cell Distribution Width as an Important Predictor of Outcome in Different Clinical Settings,” BioMed Research International (2018)
- US Preventive Services Task Force (USPSTF), Iron deficiency screening recommendations: https://www.uspreventiveservicestaskforce.org/
- LabCorp Test Menu, RDW Reference Ranges: https://www.labcorp.com/
- Quest Diagnostics Test Directory: https://www.questdiagnostics.com/





