

Abdominal pain sends more Americans to the ER than any other complaint, over 13 million visits a year, according to CDC data. Yet most patients still wait too long, hoping the next few hours will sort it out. Sometimes those hours are exactly what costs an appendix, a pregnancy, or a life.
Table of Contents
Quick Answer: Three abdominal pain warning signs require an emergency room visit. First, sudden, severe pain that does not ease within 30 minutes or comes with a rigid, board-like abdomen. Second, pain combined with high fever and persistent vomiting that prevents you from keeping liquids down. Third, pain with any sign of internal bleeding such as blood in vomit or stool, black tarry stools, or any new pain during pregnancy. If you see any of these, call 911 or go straight to the nearest ER.

At a Glance
• Abdominal pain is the #1 reason for US ER visits (about 8.9% of all visits, NHAMCS data)
• Over 13 million US ED visits each year are for stomach and abdominal pain (CDC)
• Three warning signs always mean ER: sudden severe pain, pain with fever and vomiting, pain with bleeding
• A rigid, board-like abdomen often signals a perforated organ, a true surgical emergency
• Lower right pain that started at the belly button may be appendicitis (1 in 20 Americans get it)
• New abdominal pain during pregnancy needs same-day evaluation, even if mild
• Older adults often show milder symptoms despite serious conditions; lower the threshold for them
Why Severe Abdominal Pain Is a Top US Emergency
Abdominal pain leads every published list of US emergency room chief complaints. National Hospital Ambulatory Medical Care Survey (NHAMCS) data from 2021 ranks it as the single most common reason adults walk through ER doors, representing roughly 8.9% of all visits (North American Community Hub analysis of NHAMCS).
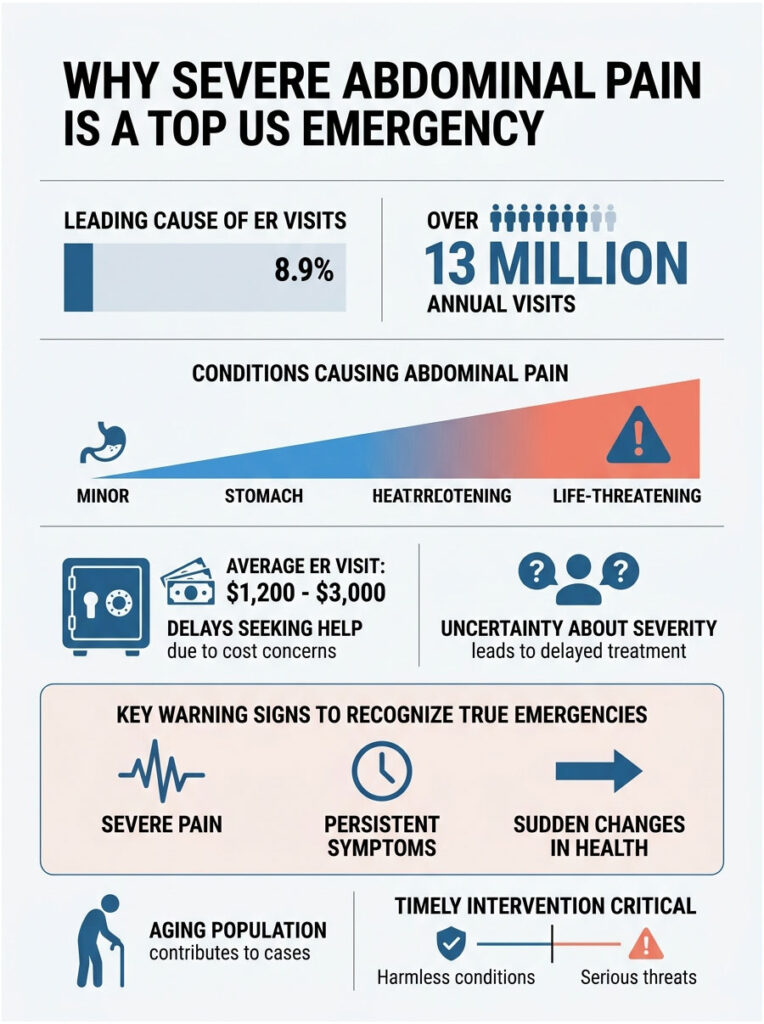
CDC tallies put that at more than 13 million annual ED visits for stomach and abdominal pain, climbing year over year as the population ages (CDC NCHS Emergency Department Summary). The conditions behind that pain range from harmless gas to a ruptured aorta, and the difference can be measured in minutes.
Why So Many Americans Wait Too Long
Cost worries drive a lot of the delay. The average US ER visit costs $1,200 to $3,000 out of pocket, and patients who carry high-deductible plans often hope the pain will pass before they have to swipe a card. Across patients booking blood panels and abdominal imaging through HealthCareOnTime, our team regularly sees CBCs and lipase tests ordered days after a pain spike that should have triggered same-day imaging.
The other driver is uncertainty. Most people have had bad gas, food poisoning, or a stomach virus before, so they tell themselves this episode is the same. Our medical reviewers note that the three warning signs below are the cleanest filter for telling true emergencies apart from passing discomfort.
Warning Sign 1: Sudden, Severe Pain That Doesn’t Ease
The first red flag is pain that arrives quickly, hits hard, and refuses to back off. The American College of Emergency Physicians (ACEP) tells patients that pain which is sudden and severe or does not ease within 30 minutes should be treated as an emergency (ACEP Stomach Pain Guidance).
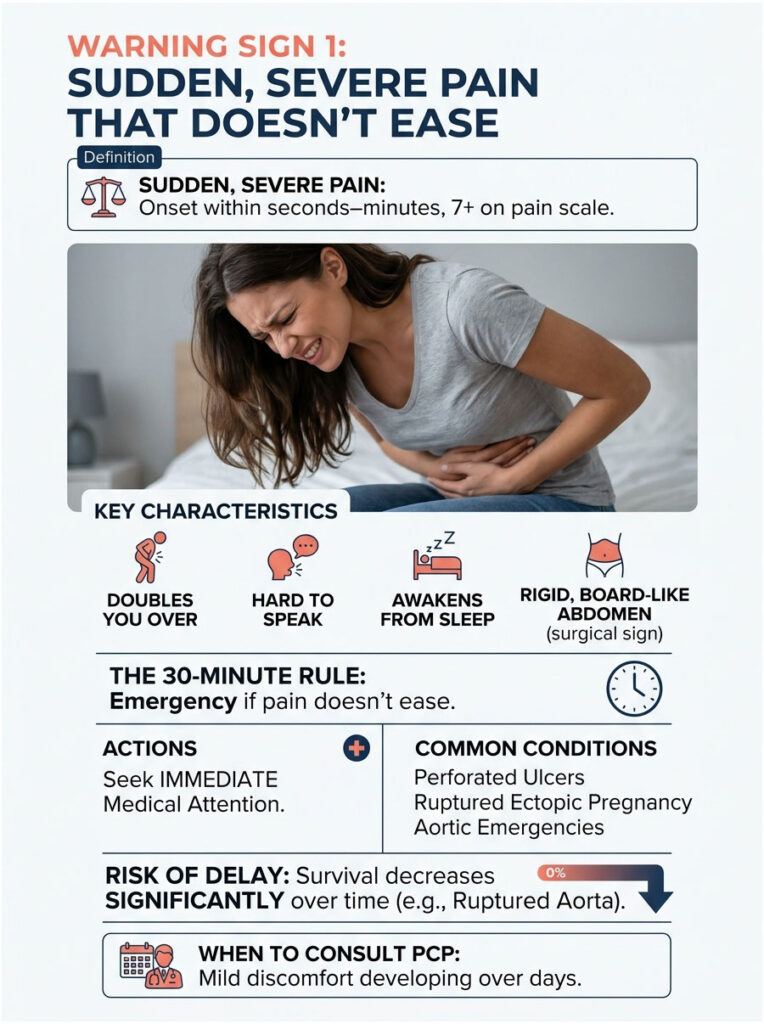
The 30-minute rule is not arbitrary. Surgical conditions that need immediate intervention (perforated ulcer, ruptured ectopic pregnancy, aortic emergencies) almost never settle on their own. If anything, they get worse fast.
What “Sudden and Severe” Actually Looks Like
Sudden means the pain came on within seconds to minutes, not hours. Many ER patients describe it as a switch flipping. Severe means a 7 or higher on a 0 to 10 scale, the kind of pain that doubles you over, makes it hard to speak in full sentences, or wakes you out of sleep.
If you cannot stand up straight, cannot find a comfortable position, or cannot focus on a conversation because of the pain, that meets the bar. Mild discomfort that grows over a day or two is a different problem and usually allows time to call a primary care provider first.
The Rigid, Board-Like Abdomen (a Surgical Red Flag)
Press gently on your own belly. A normal abdomen feels soft and gives under your fingers. A rigid, board-like abdomen feels hard, stiff, and tense even between breaths. ER physicians call this “guarding,” and it usually means the lining of the abdominal cavity (the peritoneum) is inflamed.
This finding is one of the strongest single signals of a true surgical emergency. Cleveland Clinic and Cedars-Sinai both list it among the symptoms that warrant immediate hospital evaluation (Cleveland Clinic Abdominal Pain). Do not wait it out. Get to an ER.
What Conditions This May Signal
Sudden, severe pain (especially with rigidity) commonly points to one of these emergencies:
- Perforated peptic ulcer: a hole in the stomach or duodenal wall that spills acid into the abdominal cavity
- Ruptured appendicitis: starts as dull belly-button pain, shifts to lower right, then turns sharp
- Ruptured ectopic pregnancy: pain in the lower abdomen or pelvis in someone who may be pregnant
- Abdominal aortic aneurysm (AAA) rupture: sudden severe pain in the abdomen or back, often with a pulsing sensation
- Bowel obstruction with strangulation: cramping pain, distended belly, no gas or stool
- Mesenteric ischemia: severe pain out of proportion to the physical exam findings, more common in older adults
The AAA case is the most missed of the bunch. A rupturing aorta can present as severe back-and-abdomen pain in an older smoker or hypertensive patient, and survival drops by the minute.
Warning Sign 2: Pain With Fever and Persistent Vomiting
The second red flag is pain that travels with a high fever and vomiting you cannot stop. Either symptom alone might wait until morning. Together, they almost never should.
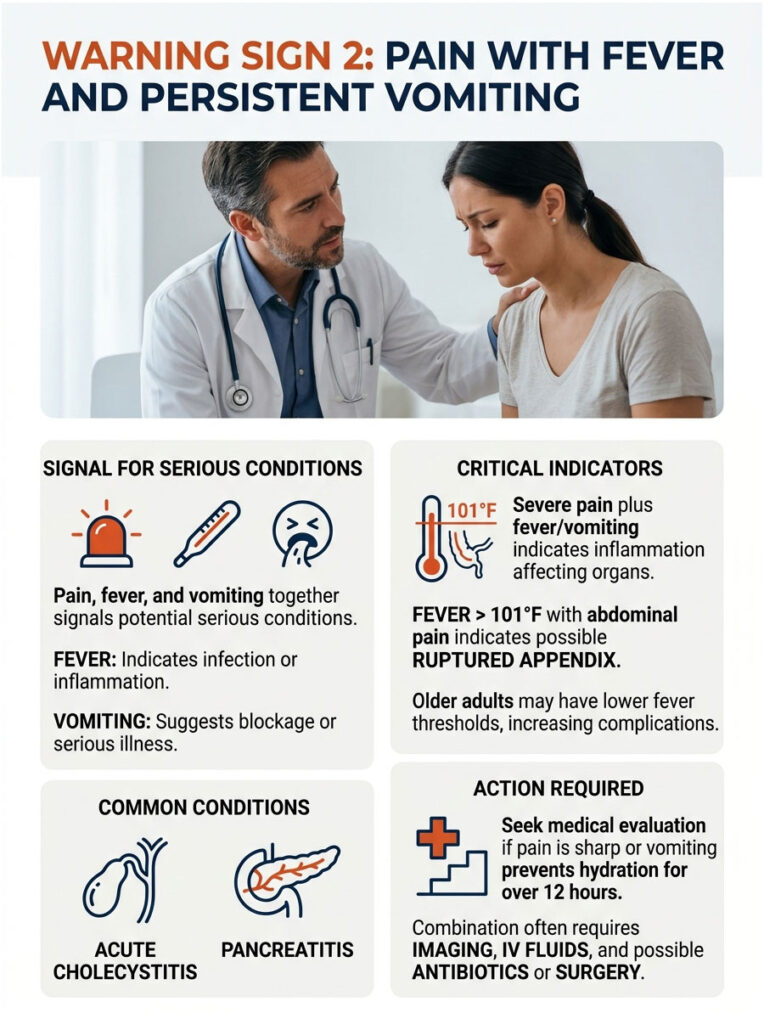
Fever signals infection or significant inflammation. Persistent vomiting suggests the gut is blocked, the pancreas is inflamed, or the body is fighting something serious. When both arrive with abdominal pain, the underlying problem usually needs imaging, IV fluids, and either antibiotics or surgery.
Why the Combination Is More Dangerous Than Either Alone
A stomach virus can produce fever and vomiting without putting a patient at real risk. The added factor is severe or localized pain. Pain plus fever plus vomiting usually means the inflammation is no longer confined to the stomach lining; it has moved to an organ (the appendix, gallbladder, pancreas) or to the peritoneal lining.
Patients commonly ask us how long they should ride out a stomach bug at home. The answer from our medical team: if pain is sharp and localized, if vomiting prevents keeping water down for more than 12 hours, or if a fever climbs above 101°F, get evaluated.
Fever Thresholds That Demand the ER
A fever between 99°F and 100.5°F is common with garden-variety appendicitis or mild gallbladder irritation. A fever above 101°F (38.3°C) paired with abdominal pain and rising heart rate is a different signal entirely. Healthline’s summary of NIH guidance notes that this combination may indicate that an inflamed appendix has ruptured (Healthline Appendicitis Emergency Symptoms).
For older adults, the threshold drops. The StatPearls Acute Abdomen monograph reminds clinicians that seniors with appendicitis or gallbladder disease often run lower fevers and show less guarding, yet have higher complication rates (NCBI StatPearls Acute Abdomen). A 99.8°F fever in a 75-year-old can mean what 102°F means in a 25-year-old.
Conditions This Often Signals
Pain plus fever plus vomiting commonly points to:
- Appendicitis with rupture: pain that started near the belly button, shifted to the lower right, then spiked
- Acute cholecystitis (gallbladder infection): severe right upper-quadrant pain lasting more than four to six hours, often after a fatty meal
- Acute pancreatitis: severe upper abdominal pain that wraps to the back, often with nausea and tachycardia
- Acute cholangitis: right upper-quadrant pain, fever, and yellowing skin (Charcot’s triad)
- Diverticulitis with abscess: cramping lower-left pain with fever
- Severe bowel infection or ischemic colitis: bloody diarrhea, fever, and worsening pain
Acute cholecystitis and acute cholangitis both feature in the StatPearls acute abdomen reference and both require prompt antibiotics and surgical consultation. A simple lipase test, available through most US labs and through HealthCareOnTime diagnostic panels, can rule pancreatitis in or out within hours.
Warning Sign 3: Pain With Internal Bleeding Signs
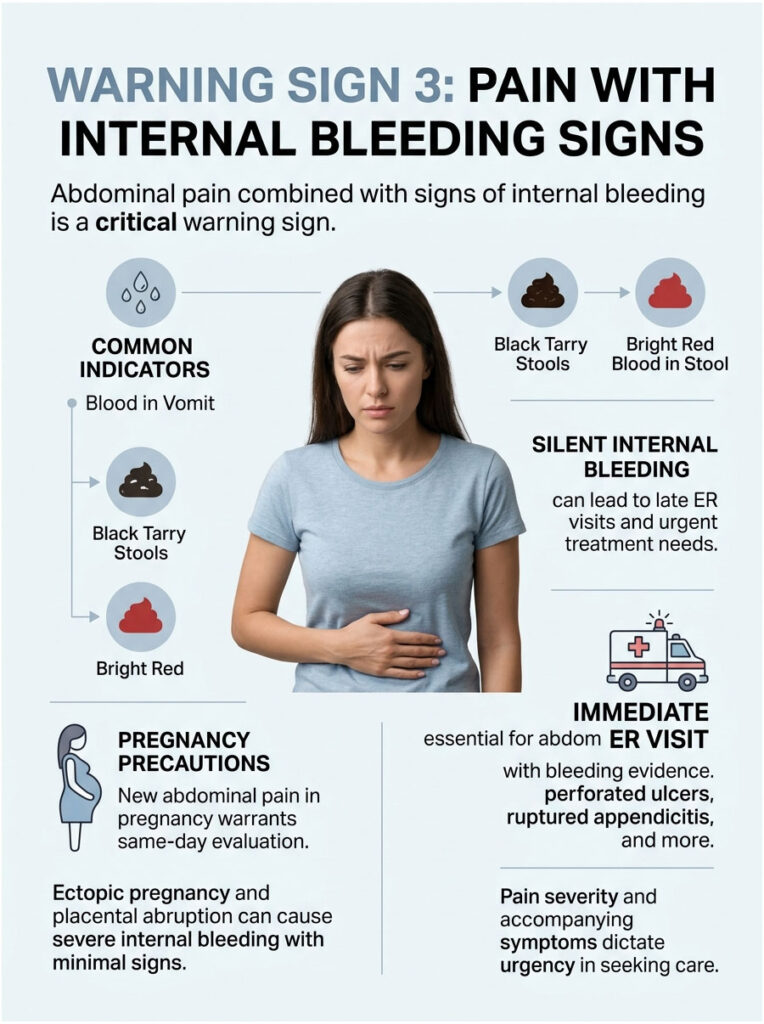
The third red flag is abdominal pain paired with any evidence that you are bleeding inside. This is the most underestimated of the three signs because the bleed itself can be silent for hours.
In cases reviewed by our medical team, patients with this combination often arrive in the ER late because they assumed the dark stool was from iron supplements or the spotting was a normal period. By the time blood pressure drops, treatment becomes urgent and the recovery longer.
Blood in Vomit, Black Tarry Stools, Bright Red Blood in Stool
Vomit that contains bright red blood or that looks like coffee grounds points to bleeding in the upper GI tract (esophagus, stomach, or duodenum). Black, tarry, foul-smelling stools (called melena) indicate digested blood, usually from an upper GI bleed. Bright red blood in the stool or in the toilet suggests a lower GI bleed.
Any of these combined with abdominal pain warrants an immediate ER visit, not a wait-and-see day. Cedars-Sinai explicitly lists stomach pain accompanied by dark or black stool, vomiting blood, or persistent vomiting as reasons to seek care right away (Cedars-Sinai on Appendicitis).
Pain During Pregnancy: a Special Subset
New abdominal pain in pregnancy needs same-day evaluation even when it feels mild. The two emergencies that drive this rule are ectopic pregnancy (a fertilized egg implants outside the uterus, most often in a fallopian tube) and placental abruption (the placenta separates from the uterine wall in the second or third trimester).
Both can cause severe internal bleeding with little outward sign at first. Spotting plus one-sided pelvic pain in early pregnancy is an ectopic until proven otherwise. Sudden severe pain plus a tense, painful uterus in late pregnancy raises concern for abruption. A beta-hCG blood test, available through most US labs and HealthCareOnTime panels, is often the first step in ER workup for any pregnant patient with new pain.
Conditions This Often Signals
Pain with bleeding evidence commonly signals:
- Perforated peptic ulcer with bleed: severe upper abdominal pain plus coffee-ground vomit or melena
- Esophageal varices rupture: vomiting bright red blood in someone with a history of liver disease
- Ectopic pregnancy: one-sided pelvic pain plus spotting plus a positive pregnancy test
- Placental abruption: third-trimester pain with vaginal bleeding and a hard, tender uterus
- Diverticular bleeding: painless or mildly painful passage of large amounts of dark red blood
- Mesenteric ischemia: severe pain plus bloody stools, more common in older patients with vascular disease
- Ruptured AAA: severe abdomen-and-back pain with shock, hidden bleeding into the abdominal cavity
Table 1: The 3 Warning Signs at a Glance
| Warning Sign | Key Features to Spot | Possible Cause | What to Do |
| Sudden, severe pain that does not ease | Onset in seconds to minutes; 7+/10 intensity; rigid, board-like abdomen; cannot find a comfortable position | Perforated ulcer, ruptured appendicitis, ruptured ectopic pregnancy, AAA rupture, mesenteric ischemia | Call 911 or go to ER immediately; do not drive yourself if pain is severe |
| Pain with high fever and persistent vomiting | Fever above 101°F (38.3°C); cannot keep liquids down for 12 hours; rising heart rate; localized tenderness | Appendicitis with rupture, acute cholecystitis, pancreatitis, cholangitis, diverticulitis with abscess | Go directly to ER; bring a list of medications; expect IV fluids and imaging |
| Pain with internal bleeding signs | Vomiting blood or coffee-ground material; black tarry stools; bright red blood in stool; spotting in pregnancy with pelvic pain | Perforated peptic ulcer with bleed, esophageal varices, ectopic pregnancy, placental abruption, diverticular bleed | Call 911 or go to ER; do not eat or drink anything; save samples if safe |
| Severe pain in older adults (65+) | Even moderate pain may signal serious illness; less fever and guarding than in younger adults | Mesenteric ischemia, perforated viscus, AAA, atypical appendicitis | Lower threshold; treat any new severe pain as urgent |
| Severe pain in pregnancy | One-sided pelvic pain plus spotting; sudden upper abdominal pain in late pregnancy | Ectopic pregnancy, placental abruption, preeclampsia, HELLP syndrome | Same-day evaluation always; call OB or go to ER |
How to Tell the Difference: Everyday Pain vs Emergency Pain
Most abdominal pain is harmless. The challenge is keeping calm enough to spot the rare episode that is not. A simple framework, drawn from US emergency medicine practice, helps separate routine from urgent.
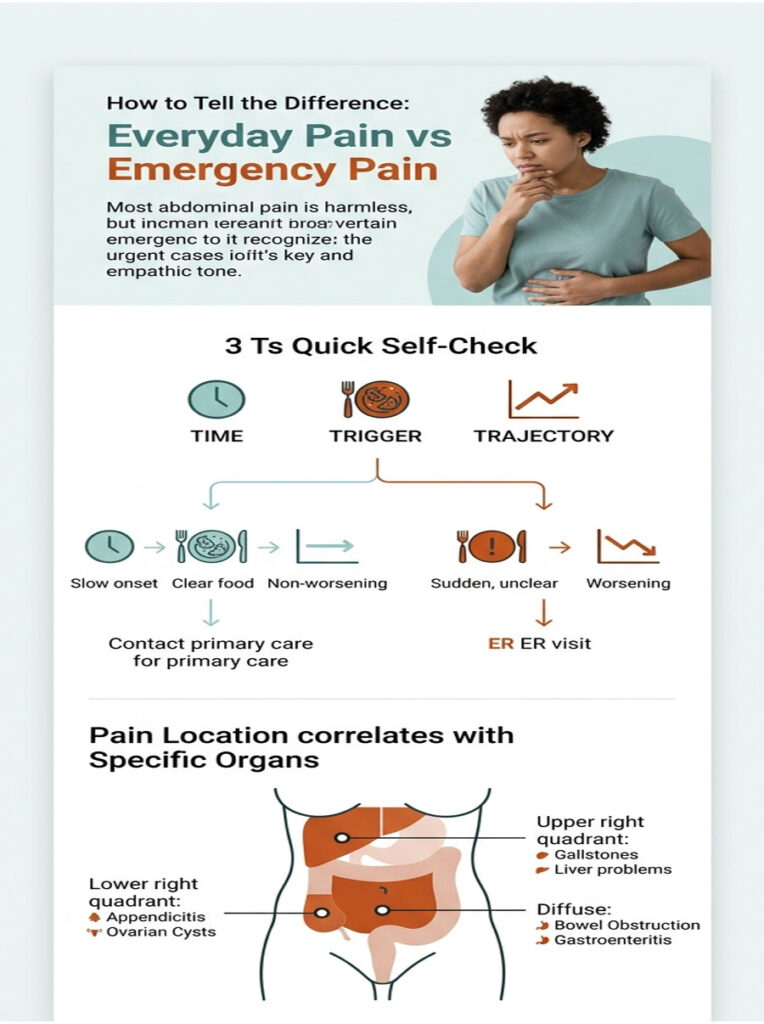
The “3 Ts” Quick Self-Check: Time, Trigger, Trajectory
The “3 Ts” frame asks three short questions any patient can answer in 30 seconds:
- Time: when exactly did the pain start? Pain that began suddenly within the last few hours is more concerning than pain that has come and gone for weeks.
- Trigger: did it follow a heavy meal, a workout, a new medication, vomiting, or a fall? A clear trigger sometimes points to a benign cause; a trigger-free onset is more suspicious.
- Trajectory: is the pain getting better, the same, or rapidly worse? Pain that climbs sharply over hours is a stronger emergency signal than steady pain that holds at the same level.
Sudden onset, no clear trigger, and a worsening trajectory together push the case toward the ER. Slow onset, a clear food trigger, and a fading trajectory usually allow a phone call to the primary care provider first.
Pain Locations and What They May Signal
Abdominal pain is not random. Certain regions tend to correlate with certain organs, and that mapping helps physicians narrow the differential quickly. The same map helps patients describe symptoms accurately to a 911 dispatcher or triage nurse.
Table 2: Where the Pain Sits and What US Doctors Look For
| Pain Location | Possible Conditions | US Diagnostic Pattern |
| Lower right quadrant | Appendicitis, ovarian cyst, ectopic pregnancy, Crohn’s disease, kidney stone | CT scan or ultrasound; appendix point tenderness (McBurney’s point); 1 in 20 Americans develop appendicitis (NIDDK) |
| Upper right quadrant | Gallstones, acute cholecystitis, hepatitis, liver abscess | Right upper-quadrant ultrasound; Murphy’s sign on exam; liver enzymes and lipase |
| Upper middle (epigastric) | Peptic ulcer, gastritis, pancreatitis, early appendicitis, heart attack | ECG to rule out cardiac cause; lipase and amylase; upper GI workup |
| Lower left quadrant | Diverticulitis, ovarian pathology, sigmoid colitis, kidney stone | CT scan; inflammatory markers; one of most common causes of left-sided pain after age 50 |
| Lower middle (suprapubic) | Bladder infection, pelvic inflammatory disease, ectopic pregnancy, uterine pathology | Urinalysis, pregnancy test, pelvic ultrasound |
| Pain that wraps to the back | Pancreatitis, kidney stone, AAA, posterior peptic ulcer | CT abdomen with contrast; lipase; AAA screening in older smokers per US Preventive Services Task Force |
| Diffuse, all-over abdominal pain | Bowel obstruction, mesenteric ischemia, gastroenteritis, peritonitis | Plain abdominal X-ray, CT scan, lactate level |
Source: synthesized from NCBI StatPearls Acute Abdomen and Mass General Brigham clinical guidance.
Demographics That Need a Lower Threshold
Standard warning signs assume an average adult. Several groups deserve a lower threshold for ER evaluation because their bodies hide serious problems behind milder symptoms.
Pregnant Patients
Any new abdominal pain in pregnancy deserves same-day evaluation. Ectopic pregnancy is the leading cause of first-trimester maternal death in the US, and the classic warning combination is one-sided pelvic pain plus vaginal spotting plus a positive pregnancy test. Later in pregnancy, severe abdominal pain may signal preeclampsia, HELLP syndrome, or placental abruption.
Patients commonly ask us whether to call their OB or go straight to the ER. The shortcut: if the pain is mild and stable, call the OB office; if severe, bleeding, or paired with dizziness, go to the ER and call the OB on the way. Across pregnant patients booking beta-hCG and CBC panels through HealthCareOnTime, our team sees the same pattern; early lab work catches ectopic pregnancies faster than waiting for an OB appointment.
Older Adults (65+)
Older patients often present atypically. They may have appendicitis without the classic fever, mesenteric ischemia without obvious tenderness, or a ruptured AAA mistaken for back strain. The StatPearls reference is explicit that seniors with serious abdominal conditions often look deceptively well at first.
Our medical reviewers see this pattern frequently in older patients undergoing pre-operative labs and CT planning. A 70-year-old with new abdominal pain that has lasted more than a few hours deserves the ER, not a “let’s see how you feel tomorrow.” Family members and home caregivers should be alert to subtle signals like loss of appetite, low-grade confusion, or refusal to walk, any of which may precede a more obvious abdominal complaint.
Children Under 5
Young children cannot describe pain location or quality well. Warning signs in toddlers include refusing food, persistent crying, drawing the knees up to the chest, vomiting bile (green), or a swollen, tender belly. Intussusception (one part of the bowel telescoping into another) classically presents with episodic severe pain plus “currant jelly” stools.
Any of these in a child under 5 should prompt a pediatric ER visit. Adult ERs see kids too, but pediatric-equipped facilities (where available) are better staffed for abdominal emergencies in children. A parent’s instinct that “something is wrong” matters more than a normal-looking temperature reading.
Immunocompromised Patients
People on chemotherapy, long-term steroids, biologics for autoimmune disease, or anti-rejection drugs after a transplant often cannot mount a normal inflammatory response. They may have appendicitis or perforation with little fever and almost no abdominal rigidity.
For this group, any moderate-to-severe abdominal pain deserves same-day medical evaluation. Across patients reviewed by our medical team, the immunocompromised group is the one where waiting most often turns a fixable problem into a critical one. Routine inflammatory markers (CRP, procalcitonin) that HealthCareOnTime panels include are useful early signals when classic fever and pain patterns are blunted.
ER vs Urgent Care vs Primary Care: Where to Go
The right care setting depends on severity, the presence of warning signs, and the patient’s underlying risk. Mass General Brigham urgent care medical director Ronak V. Shah, MD, advises that any abdominal pain that is brand new or severe deserves an in-person evaluation, with the ER reserved for true red flags (Mass General Brigham).
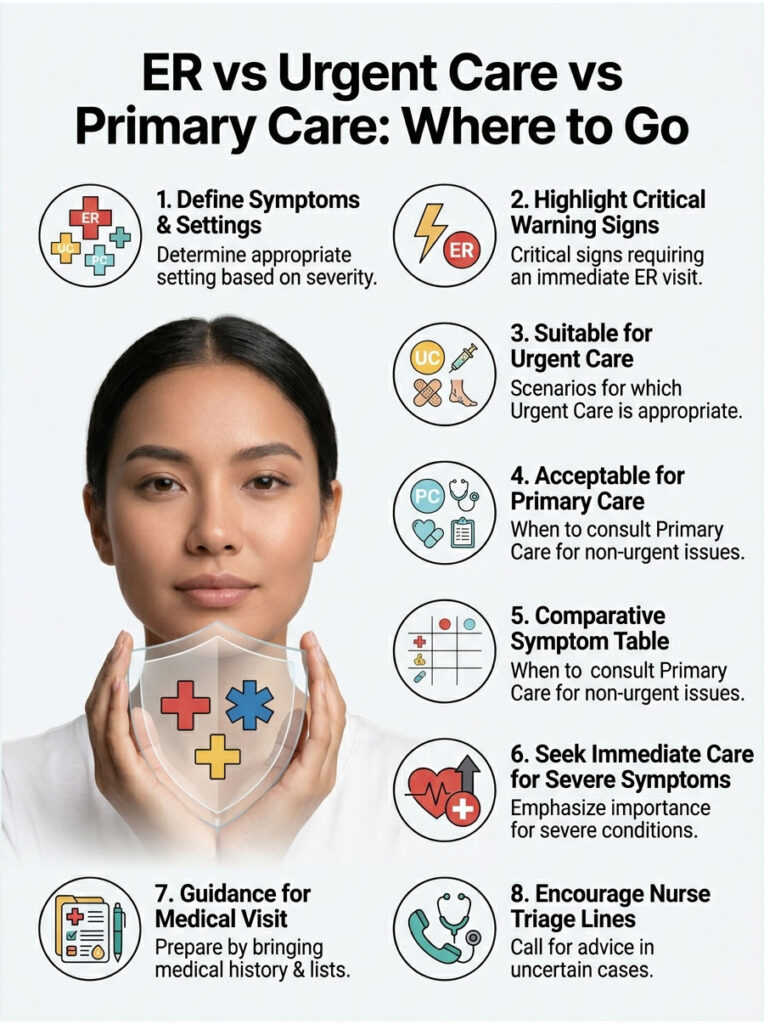
When the ER Is the Only Right Answer
Go to the ER (or call 911 if pain is incapacitating or you cannot get there safely) for any of the three warning signs above, for severe pain that lasts more than 30 minutes, for any new abdominal pain in pregnancy that is severe or bleeding-associated, and for any abdominal pain after major trauma.
When Urgent Care Is Reasonable
Urgent care can handle moderate, non-red-flag pain that has lasted more than a day, mild gastroenteritis with stable vital signs, suspected urinary tract infections, and mild flares of known chronic conditions. Most US urgent care centers have basic labs and X-ray but not CT, so anything needing advanced imaging gets transferred to the ER.
When Calling the Doctor Is Fine
Stable, mild pain that has gone on for several days without fever, bleeding, or vomiting can usually wait for a primary care call. The same applies to recurring pain you have had evaluated before and know the cause of. When in doubt, call a nurse triage line; most US insurance plans offer one.
Table 3: Symptom Scenario / Recommended Action
| Patient Scenario | Best Care Setting | Suggested Next Step |
| Sudden severe pain plus rigid abdomen | ER (call 911 if cannot get there safely) | Do not eat or drink; arrange immediate transport |
| Pain plus fever above 101°F plus persistent vomiting | ER | Bring medication list; expect IV fluids and CT scan |
| Pain plus blood in vomit, black or bright red stool | ER | Do not eat or drink; save samples if safe to do so |
| New pain in pregnancy (any trimester) | ER or OB office same day | Call OB on the way; do not delay if pain is severe |
| Moderate pain over 24 hours, stable vital signs, no red flags | Urgent care or primary care same day | Hydrate; track symptoms; bring a symptom log |
| Mild, recurring pain you have had evaluated before | Primary care call within a few days | Check whether prior workup needs an update |
What Happens in the ER for Severe Abdominal Pain
Knowing what to expect can shorten the time between arrival and treatment. US emergency departments follow a standard sequence for abdominal pain that has been refined over decades of practice.
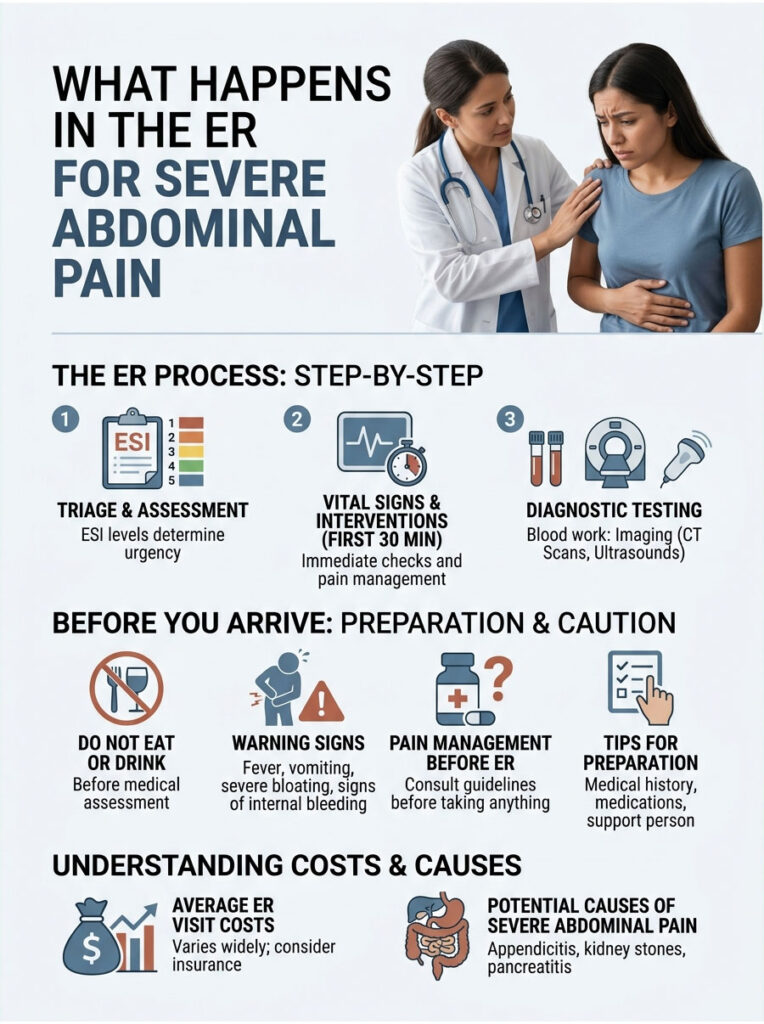
Triage, Vital Signs, and the First 30 Minutes
Triage nurses use the Emergency Severity Index (ESI) to assign acuity. Patients with severe pain, low blood pressure, or signs of internal bleeding usually score ESI 1 or 2 and go straight to a room. Vital signs (heart rate, blood pressure, temperature, oxygen, respiratory rate) get checked within minutes.
An IV line goes in early, both to draw blood and to deliver fluids or medication if needed. Pain medication is usually given before a full diagnosis because withholding analgesia does not change exam accuracy, per current US emergency medicine practice.
Common Tests: Blood Work, CT Scan, Ultrasound
Blood tests typically include a complete blood count (CBC) to check for infection, a basic metabolic panel for kidney function, lipase for pancreatitis, liver enzymes, lactate for tissue ischemia, and a pregnancy test in any patient of childbearing age. Urine is usually checked for infection, blood, and pregnancy.
Imaging depends on the suspected diagnosis. A CT scan of the abdomen and pelvis (with contrast unless contraindicated) is the workhorse for unexplained severe pain. Ultrasound is preferred for suspected gallbladder, pregnancy, or pediatric appendicitis cases.
Average US ER Costs and How to Prepare
The average US emergency room visit runs $1,200 to $3,000 out of pocket before insurance, with imaging and admission pushing it higher. Bringing your ID, insurance card, an updated medication list, and a brief written summary of your symptoms (when they started, what they feel like, what makes them better or worse) speeds intake.
Skip eating or drinking from the moment you decide to go to the ER, in case surgery is needed. If you live alone, call a friend or family member to meet you; abdominal pain can worsen quickly and you may need someone to drive you home or stay overnight.
Frequently Asked Questions
What are the 3 warning signs of severe abdominal pain?
The three warning signs are: sudden severe pain that does not ease within 30 minutes (especially with a rigid, board-like abdomen), pain combined with high fever and persistent vomiting, and pain paired with any sign of internal bleeding like blood in vomit, black tarry stools, or new pain during pregnancy. Any of these means call 911 or go to the ER.
How long is too long for severe abdominal pain?
Severe pain that has not eased within 30 minutes is already too long, per ACEP guidance. Even moderate pain that lasts more than a few hours and is getting worse deserves evaluation. Pain that disrupts sleep, prevents you from keeping fluids down, or makes you double over is an ER trip regardless of how long it has lasted.
Can severe abdominal pain be a heart attack?
Yes, especially in older adults, women, and people with diabetes. Heart attacks can present as upper abdominal or epigastric pain, sometimes with nausea, sweating, and shortness of breath. ER physicians often run an ECG even for upper abdominal pain in higher-risk patients. Call 911 if pain is severe and paired with chest pressure, jaw or arm pain, or sudden sweating.
What does appendicitis pain feel like in the first few hours?
Classic appendicitis starts as a dull ache near the belly button. Over 6 to 24 hours, the pain shifts to the lower right abdomen and becomes sharper, especially with movement, coughing, or sneezing. Loss of appetite, nausea, and a low-grade fever often follow. About 1 in 20 Americans develop appendicitis, so this pattern deserves an ER trip.
Is it normal to have sharp stomach pain after eating?
Mild, brief discomfort after a heavy or fatty meal is common. Sharp, severe pain after eating, especially in the right upper quadrant, may signal gallstones or acute cholecystitis. Recurring sharp pain after meals deserves a primary care or gastroenterology workup. New severe pain after eating that lasts more than four hours warrants ER evaluation.
When should I go to the ER for stomach pain in pregnancy?
Any severe abdominal pain in pregnancy warrants same-day evaluation. Go to the ER for severe pain, pain with bleeding or spotting, sudden one-sided lower abdominal pain, pain with dizziness or fainting, or pain in the third trimester paired with a tense, painful uterus. For mild stable pain, calling the OB office first is reasonable.
Should I take painkillers before going to the ER?
It is best to skip over-the-counter NSAIDs (ibuprofen, naproxen, aspirin) before an ER visit because they can worsen GI bleeding and mask symptoms. Acetaminophen (Tylenol) is generally safer, but if pain is severe enough to drive an ER visit, ER staff can give stronger, faster medication on arrival. Do not eat or drink either, in case surgery is needed.
What causes a rigid, board-like abdomen?
A rigid abdomen usually means the peritoneum (the lining of the abdominal cavity) is inflamed, a condition called peritonitis. Causes include a perforated ulcer, ruptured appendix, ruptured ectopic pregnancy, severe pancreatitis, or bowel perforation. This finding is one of the strongest signals of a true surgical emergency and warrants an immediate ER visit.
Is severe abdominal pain at night more serious?
Pain that wakes you from sleep or starts in the middle of the night is generally considered more concerning than daytime pain. Night-time pain is less likely to be functional (stress-related or food-related) and more likely to reflect an organic problem. If severe abdominal pain wakes you up, do not try to sleep it off; evaluate the three warning signs and act.
Can I drink water if my stomach pain is severe?
It is safer not to. Severe abdominal pain that may need surgery, imaging with contrast, or endoscopy usually requires an empty stomach. Drinking water or eating before ER arrival can delay anesthesia and treatment. Wait until ER staff clear you to drink, which usually happens once the cause is clearer or surgery is ruled out.
How is bowel obstruction diagnosed in the ER?
ER teams suspect bowel obstruction in patients with severe cramping pain, abdominal distension, persistent vomiting, and no passage of gas or stool, especially with a history of prior abdominal surgery or hernia. Diagnosis usually involves an abdominal X-ray followed by CT scan. Treatment ranges from IV fluids and bowel rest to surgery, depending on cause and severity.
What is an abdominal aortic aneurysm and why is it dangerous?
An abdominal aortic aneurysm (AAA) is a bulge in the main artery running through the abdomen. When it ruptures, it causes sudden severe abdominal or back pain plus rapidly dropping blood pressure and is fatal in over half of cases. Older smokers, men over 65, and people with high blood pressure are at highest risk. The US Preventive Services Task Force recommends screening for men aged 65 to 75 with smoking history.
Disclaimer: This article is educational and does not replace personalized medical advice. If you suspect any of the three warning signs above, call 911 or go to the nearest emergency room. Do not try to diagnose severe abdominal pain at home. In the US, the Poison Help line is 1-800-222-1222 if pain may be related to a substance or overdose. If you are uncertain whether your symptoms are an emergency, call your insurance plan’s 24-hour nurse triage line or your primary care provider.
References
- CDC NCHS: Emergency Department Visits in the United States, 2016-2022
- Cleveland Clinic: Abdominal Pain Causes, Types and Treatment
- Mayo Clinic: Abdominal Pain When to See a Doctor
- American College of Emergency Physicians: Stomach Pain Know When to Go
- NCBI StatPearls: Acute Abdomen
- Mass General Brigham: Abdominal Pain ER or Urgent Care
- Healthline: Appendicitis Emergency Symptoms
- Cleveland Clinic: Appendicitis Signs Symptoms Causes Diagnosis Treatment
- Cedars-Sinai: Identifying Appendicitis
- University of Utah Health: When to Visit the ER with Abdominal Pain





