

Two people can have a hernia the size of a grape. One can safely watch it for a decade. The other belongs in an operating room within the month. The difference is not the size of the bulge. It is where the bulge sits.
Table of Contents
Quick Answer: There are seven main hernia types: inguinal, femoral, umbilical, incisional, ventral or epigastric, hiatal, and a small group of rare ones. Most are repaired surgically with mesh, either open or laparoscopically. Femoral and paraesophageal hiatal hernias need prompt repair. Inguinal and small umbilical hernias can sometimes be watched, though most eventually come to surgery anyway.
At a Glance
- Inguinal hernias make up 75% of all abdominal wall hernias, with a lifetime risk of 27% in men and 3% in women.
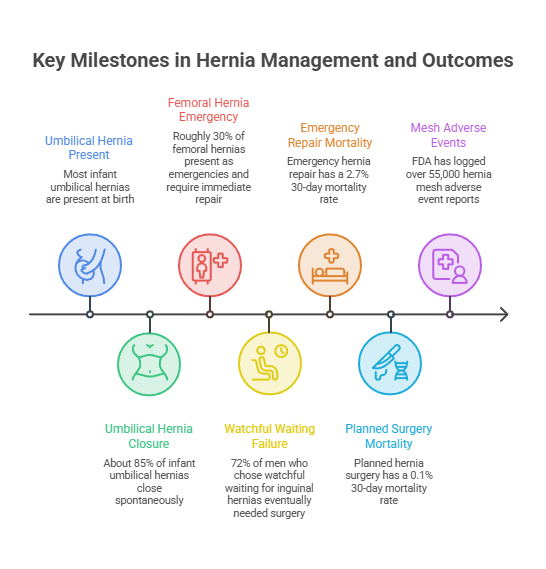
- Roughly 30% of femoral hernias present as an emergency, and they should be repaired on diagnosis even without symptoms.
- Emergency hernia repair carries a 30-day mortality of 2.7% against 0.1% for planned surgery.
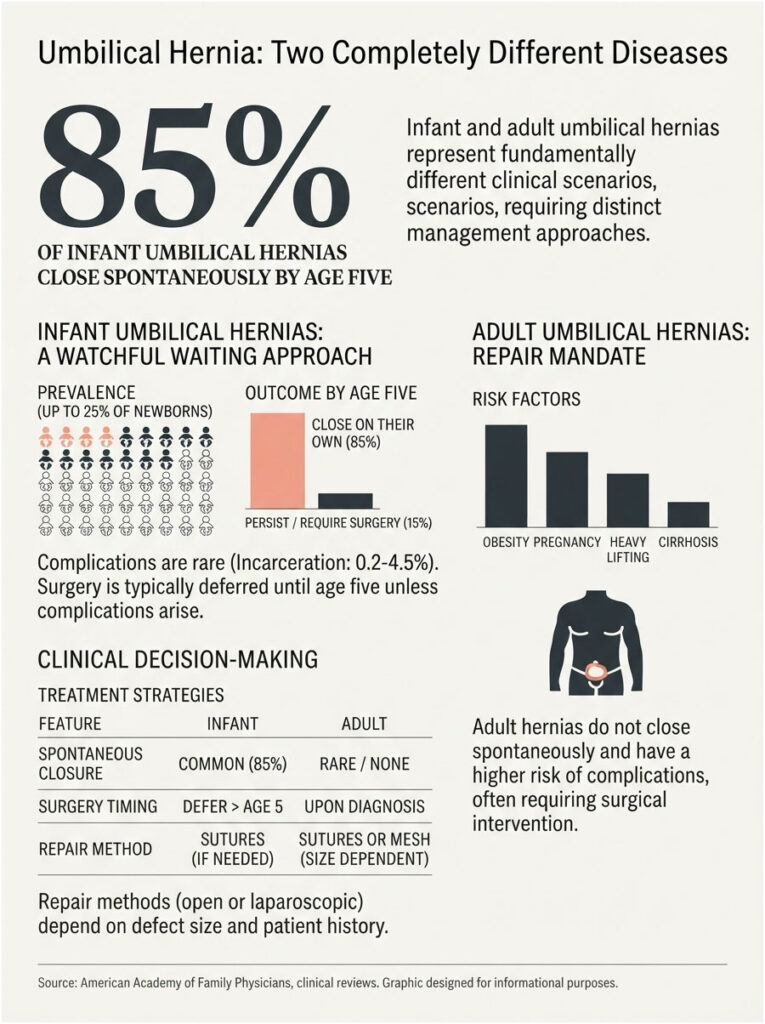
- About 85% of infant umbilical hernias close on their own by age 5. Adult umbilical hernias essentially never do.
- In long-term follow-up, 72% of men who chose watchful waiting still ended up in surgery within 7.5 years.
- FDA has logged over 55,000 hernia mesh adverse event reports, with recurrence ranging from 0% to 11.1% across the literature.
- No adult hernia heals itself. The muscle wall has no mechanism for knitting a hole shut.
The 7 Types, in One Screen
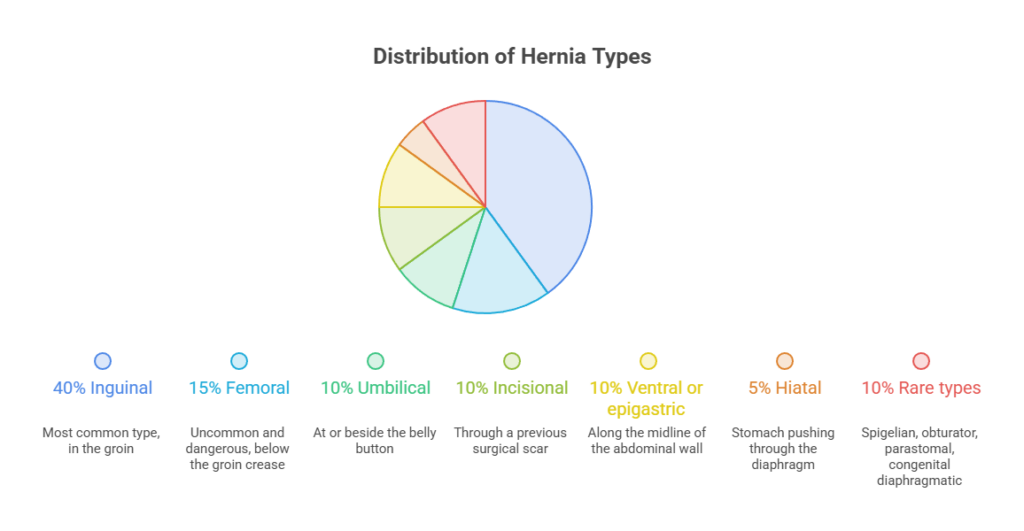
- Inguinal: groin, above the crease. The most common by a wide margin.
- Femoral: groin, below the crease. Uncommon, and the most dangerous of the everyday types.
- Umbilical: at or beside the belly button.
- Incisional: through the scar of a previous abdominal operation.
- Ventral or epigastric: anywhere along the midline of the abdominal wall.
- Hiatal: stomach pushing up through the diaphragm. Invisible from the outside.
- Rare types: Spigelian, obturator, parastomal, congenital diaphragmatic.
Which Hernias Need Surgery Now, and Which Can Wait
This is the question behind almost every hernia search, so here it is in one place.
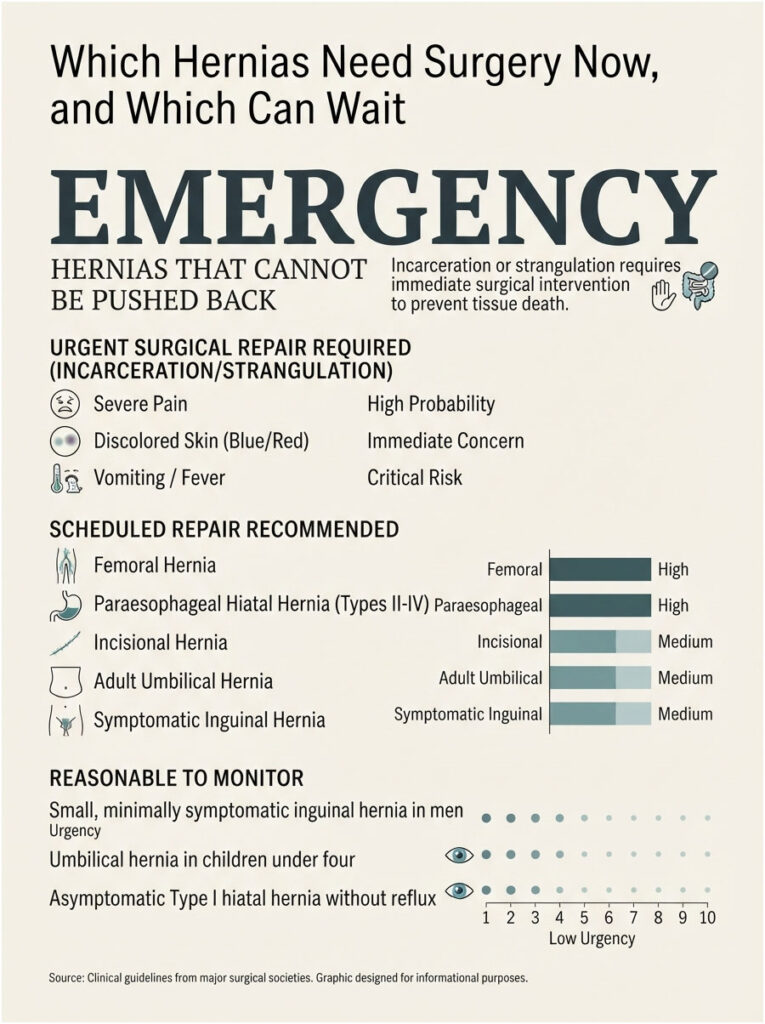
Repair now, today, no negotiation. Any hernia you cannot push back in, any hernia with sudden severe pain, discolored skin, vomiting, or fever. That is incarceration or strangulation, and the tissue inside is on a clock.
Repair soon, on a schedule. Femoral hernias (repair on diagnosis, symptoms or not), paraesophageal hiatal hernias (Types II through IV), incisional hernias, adult umbilical hernias, and any inguinal hernia causing real symptoms.
Reasonable to watch. A small, minimally symptomatic inguinal hernia in a man. An umbilical hernia in a child under four. An asymptomatic Type I hiatal hernia with no reflux.
Everything below explains why each falls where it does.
What a Hernia Actually Is (and Why It Won’t Close on Its Own)
Every hernia needs three ingredients: a weak spot in a muscle or fascia wall, pressure pushing against it, and tissue that finds the gap.

Fascia is the tough connective sheet that holds your organs in place. When it tears or thins, fat or a loop of bowel pushes through, and that push creates the bulge you can see or feel.
Here is the part patients rarely hear said plainly. In adults, that hole does not close. Fascia has no repair mechanism for a defect under constant pressure, which is why hernias grow over time and never shrink.
Reducible, incarcerated, strangulated
Three words describe a hernia’s progression, and they determine how fast you need care.
Reducible means the bulge slides back in with gentle pressure, or disappears when you lie flat. Most hernias start here and many stay here for years.
Incarcerated means the tissue is stuck. It will not go back, it hurts, and it can obstruct the bowel.
Strangulated means trapped tissue has lost its blood supply. Cells begin dying within hours. This is an emergency, not a next-week problem.
Our medical reviewers note that most people who reach an emergency room with a strangulated hernia had known about the bulge for months or years. The bulge did not suddenly change. Their luck did.
The 7 Hernia Types Side by Side
Find your row, then read the section that matches.
| Hernia Type | Where It Shows Up | Who Gets It Most | First-Line Treatment | Urgency | Key Risk |
| Inguinal | Groin, above the crease | Men (27% lifetime risk) | Mesh repair, open or laparoscopic | Elective in most cases | Progression, incarceration |
| Femoral | Groin, below the crease, upper thigh | Women (about 70% of cases) | Prompt mesh repair on diagnosis | Repair when diagnosed | Strangulation, rigid narrow neck |
| Umbilical (adult) | At or beside the navel | Adults with obesity, pregnancy history, cirrhosis | Mesh or suture repair | Elective, but do not delay | Enlargement, incarceration |
| Umbilical (infant) | Navel | Up to 25% of newborns | Observation to age 4 or 5 | Watch, rarely operate | Very low (incarceration 0.2% to 4.5%) |
| Incisional | Through a previous surgical scar | Anyone with prior abdominal surgery | Mesh repair, often robotic | Elective, repair before it grows | Enlargement, bowel involvement |
| Ventral or epigastric | Midline of the abdominal wall | Adults with raised abdominal pressure | Mesh repair if symptomatic | Elective | Pinched fat, steady growth |
| Hiatal (Type I) | Stomach sliding through the diaphragm | Adults over 50; 15% to 20% of Western adults | Acid medication and lifestyle change | Usually no surgery | Reflux, esophageal damage |
| Hiatal (Types II to IV) | Stomach beside the esophagus in the chest | Older adults, more often women | Surgical repair with fundoplication | Repair recommended | Incarceration, gastric volvulus |
Inguinal Hernia: The Most Common Type by Far
An inguinal hernia forms in the inguinal canal, the passage running through the lower abdominal wall in the groin.
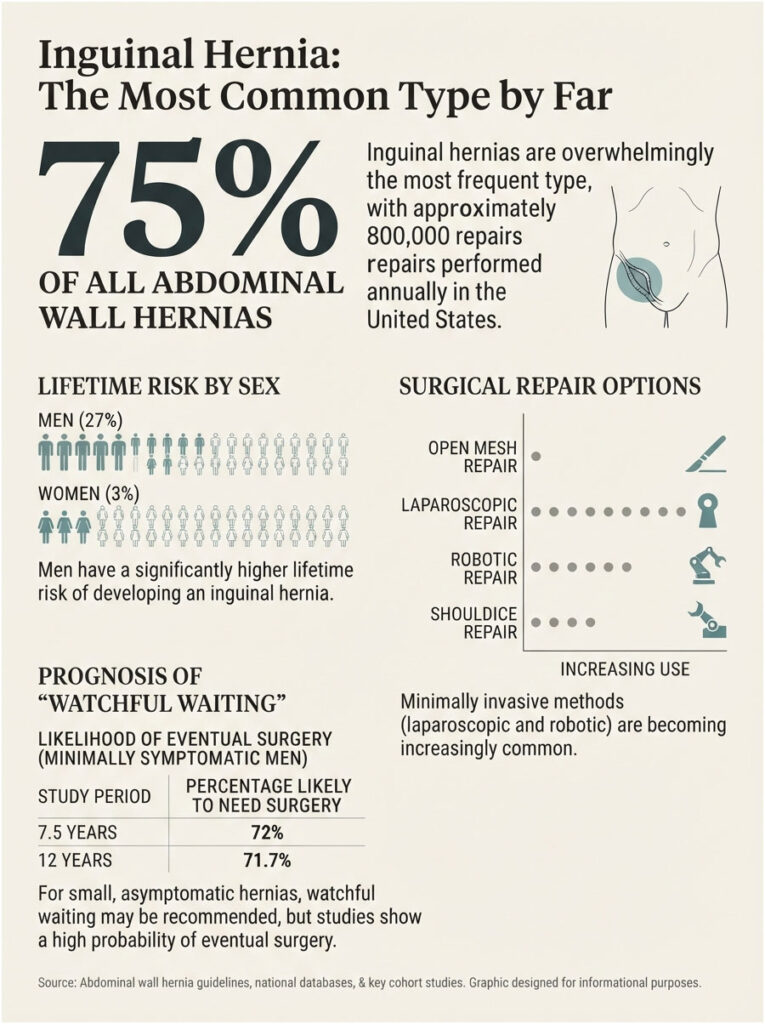
They are common on a scale that surprises people. Inguinal hernias account for about 75% of all abdominal wall hernias, and roughly 800,000 are repaired in the United States each year.
The lifetime risk is 27% in men and 3% in women. Better than one man in four will develop one.
What it feels like
A bulge in the groin that appears when you cough, strain, stand, or lift, and often vanishes when you lie down.
The sensation is usually dragging, aching, or pressure rather than sharp pain. Discomfort worsens through the day and eases with rest.
In men, a larger hernia can extend downward into the scrotum, producing visible swelling.
Direct versus indirect
An indirect hernia travels down the inguinal canal along the path the testicle took during fetal development. A direct hernia pushes straight through a weakened back wall of the canal.
About two-thirds are indirect. For you as a patient, the distinction changes almost nothing, because the surgeon covers both defects with the same repair.
Who gets them
Risk climbs with age, male sex, smoking, family history, connective tissue disorders, and anything that raises abdominal pressure, including chronic cough and straining.
The age curve is bimodal, peaking around age 5 and again after 70. Repair frequency rises from 0.25% at age 18 to 4.2% at ages 75 to 80.
How it is treated
Surgery is the only definitive fix. The two families of repair are open and minimally invasive.
Open mesh repair (Lichtenstein) lays a flat mesh sheet over the defect through a groin incision. It remains a reference standard and can be done under local or spinal anesthesia, which matters for high-risk patients.
Laparoscopic repair (TEP or TAPP) uses three small incisions and places mesh behind the muscle wall. It requires general anesthesia and is particularly useful for hernias on both sides, or for a recurrence after a previous open repair.
Robotic repair is a laparoscopic repair driven by robotic instruments. More than half of US inguinal repairs are now minimally invasive, and roughly one in five of those is robotic.
Shouldice repair layers the patient’s own tissue with no mesh at all. It is a legitimate option in specialized centers for younger, thinner patients who want to avoid an implant.
The watchful waiting trap
If your hernia is small and barely bothers you, a surgeon may offer to watch it. That offer is evidence-based, and it is routinely misunderstood.
The landmark JAMA trial led by Fitzgibbons found watchful waiting was safe for minimally symptomatic men. The long-term follow-up then found that 72% of those men were predicted to cross over to surgery by 7.5 years anyway. A separate 12-year European trial found 71.7%.
Watchful waiting rarely avoids surgery. It postpones surgery, and it postpones it into a decade when you may be older, frailer, and a worse operative candidate than you are today.
Femoral Hernia: The One That Cannot Wait
A femoral hernia pushes through the femoral canal, which sits just below the groin crease near the top of the inner thigh.
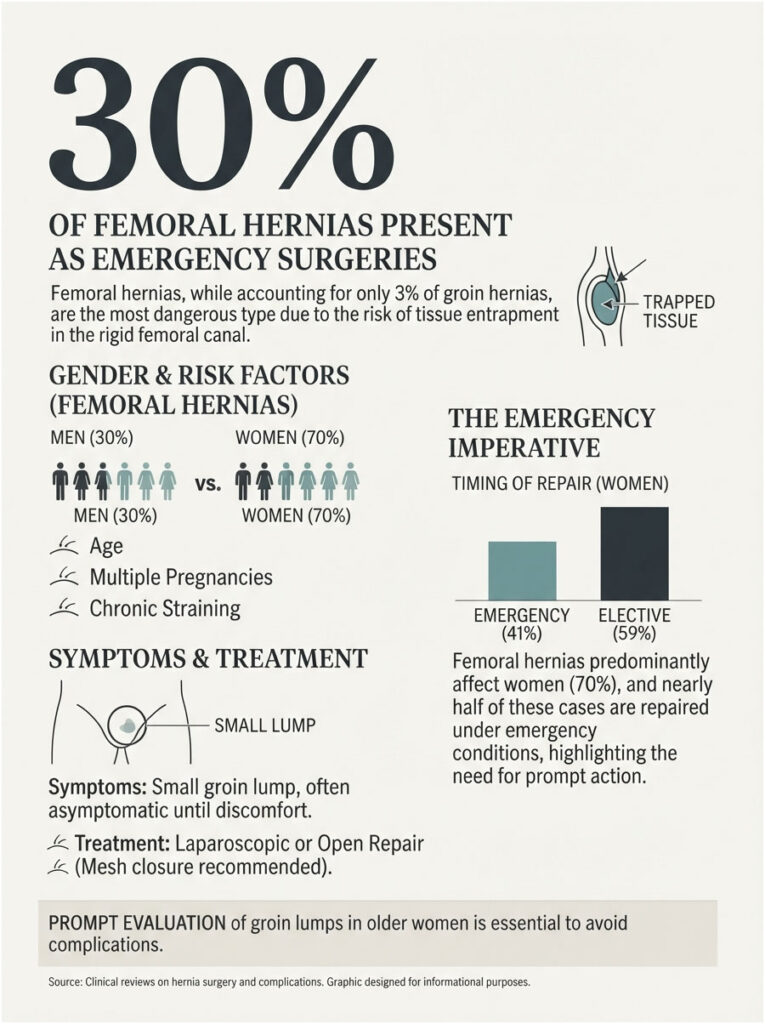
It is uncommon, making up roughly 3% of groin hernias. It is also the most dangerous of the everyday types, and the reason is pure anatomy.
Why the anatomy is the danger
The femoral canal is a narrow tunnel with rigid bony and ligamentous walls. Tissue that enters it has no room to slide back out.
An inguinal hernia has a soft, forgiving neck. A femoral hernia has a tight, unforgiving one. That single structural fact explains everything that follows.
What it feels like
A small lump low in the groin or at the very top of the inner thigh, often no larger than a marble.
It is frequently asymptomatic until it is not. Discomfort can appear when walking or climbing stairs, and it is easily mistaken for a swollen lymph node or a groin strain.
Who gets them
About 70% occur in women, and risk rises with age, multiple pregnancies, and chronic straining.
They are also easy to miss on exam because the bulge is small and sits lower than most people expect.
How it is treated
Repair is recommended once a femoral hernia is diagnosed, even when it causes no symptoms. Watchful waiting is not the standard of care here.
The data explain why. Roughly 30% of femoral hernias present as an emergency. In the Swedish Hernia Register, 41% of femoral hernias in women were repaired as emergencies, against 8.1% of inguinal hernias in women.
Repair is usually laparoscopic or open with mesh, closing the femoral canal so nothing can re-enter it.
In cases reviewed by our medical team, a groin lump in an older woman is treated as a possible femoral hernia until imaging proves otherwise. That one assumption prevents most bad outcomes in this category.
Umbilical Hernia: Two Completely Different Diseases
The same two words describe two conditions with opposite treatment plans. Age decides which one applies.
In babies, waiting is usually right
Up to 25% of newborns have an umbilical hernia, and roughly 85% close on their own by age five.
Complications are genuinely rare. Incarceration is estimated at 0.2% to 4.5%, and strangulation at under 0.8%.
The American Academy of Family Physicians advises against referring most children to a pediatric surgeon before age four or five. Taping, coins, and belly binders do not accelerate closure and can damage skin.
When a child’s hernia does need repair
Surgery becomes appropriate when the hernia persists beyond age four or five, when the fascial defect is larger than roughly 1 to 1.5 cm at ages three to four, when it is visibly enlarging, or when complications appear.
Defects under 1 cm close on their own most reliably. Defects over 2 cm rarely close before age four.
In adults, waiting is not right
An adult umbilical hernia does not close spontaneously. It enlarges, and the contents can shift from fat to bowel over time.
Risk climbs with obesity, pregnancy, heavy lifting, and cirrhosis with abdominal fluid. Patients with cirrhosis face a real risk of hernia rupture, which is why they are repaired rather than watched.
How adult repair works
Very small defects can be closed with sutures alone. Most adult repairs now use mesh, which cuts recurrence substantially, placed open or laparoscopically depending on size and prior surgery.
Incisional and Ventral Hernias: The Ones Surgery Creates
An incisional hernia forms through the scar of a previous abdominal operation. It accounts for roughly 10% of all hernias.
The mechanism is simple and a little unfair. The fascia was cut, then stitched, then healed as scar. Scar is weaker than the tissue it replaced, and abdominal pressure eventually finds the weakness.
What it feels like
A bulge along an old surgical scar that becomes obvious when you stand, cough, or strain, and often flattens when you lie down.
Aching, pulling, and a sense of pressure are common. Large incisional hernias can genuinely limit posture and activity.
What raises the risk
Obesity, active smoking, poorly controlled diabetes, a wound infection after the first surgery, and repeat operations through the same incision.
Patients booking pre-surgical panels with us often ask whether these factors still matter once the hernia exists. They matter enormously before the next repair, because they are the same factors that drive recurrence after it.
Ventral and epigastric hernias
A ventral hernia is any hernia through the front abdominal wall. An epigastric hernia sits on the midline between the navel and the breastbone, and often contains nothing but fat.
Small epigastric hernias can be startlingly painful for their size, because fat gets pinched in a tight defect with nowhere to go.
How they are treated
Small defects can be closed primarily. Larger ones need mesh. Large or complex ones may need component separation, in which the surgeon releases layers of the abdominal wall so the gap can close without tension.
Robotic repair has become common here. A meta-analysis found robotic ventral hernia repair lowered the rate of repeat surgery compared with standard laparoscopic repair and shortened hospital stay by about half a day.
Hiatal Hernia: The One You Cannot See or Feel
This is the odd one out. There is no lump to find, because the hernia sits inside your chest.
The esophagus passes through an opening in the diaphragm called the hiatus. When that opening widens, the stomach can slide or push upward into the chest cavity.
Prevalence in Western populations runs roughly 15% to 20%, and most cases produce no symptoms at all.
What it feels like
Heartburn, regurgitation, a sour taste, chest discomfort, and a burning sensation that worsens when lying down or bending forward.
Larger hernias can cause trouble swallowing, early fullness after small meals, shortness of breath, and unexplained anemia from slow bleeding.
The four types, plainly
Type I (sliding) is over 95% of all hiatal hernias. The junction of esophagus and stomach slides up and down through the hiatus.
Type II (true paraesophageal) keeps the junction anchored while the top of the stomach herniates up alongside the esophagus.
Type III (mixed) combines both patterns and makes up roughly 90% of paraesophageal hernias.
Type IV (giant) involves other organs, such as colon or spleen, entering the chest.
Types II through IV together are called paraesophageal hernias, and they represent under 5% of hiatal hernias.
Type I: medication and lifestyle first
Surgery is not recommended for an asymptomatic Type I hiatal hernia without reflux. Treatment targets the reflux, not the anatomy.
That means proton pump inhibitors or H2 blockers, weight loss, smaller meals, no food within three hours of lying down, elevating the head of the bed, and cutting alcohol and tobacco.
Types II to IV: surgery is the answer
A paraesophageal hernia carries a real risk of the stomach twisting on itself or becoming trapped. For these types, the hernia itself is the indication for repair.
The operation returns the stomach to the abdomen, removes the hernia sac, and narrows the hiatus with sutures, sometimes reinforced with mesh.
SAGES guidelines conditionally recommend adding a fundoplication during repair of Type II, III, and IV hernias, because it improves reflux control, lowers recurrence, and reduces leak risk.
Nissen, Toupet, LINX, and TIF
Nissen fundoplication wraps the top of the stomach a full 360 degrees around the esophagus and is the most widely used technique.
Toupet is a partial posterior wrap, used when swallowing is already impaired, because a full wrap can make dysphagia worse.
LINX places a ring of magnetic beads around the esophagus that opens for food and closes against reflux.
TIF is performed entirely through the mouth, with no external incisions, in selected patients with smaller hernias.
The Rarer Hernias Worth Knowing About
Spigelian hernia pushes through the Spigelian fascia along the outer edge of the rectus muscle. It often hides beneath an intact outer muscle layer, which is why it is frequently missed on exam and usually needs imaging to find.
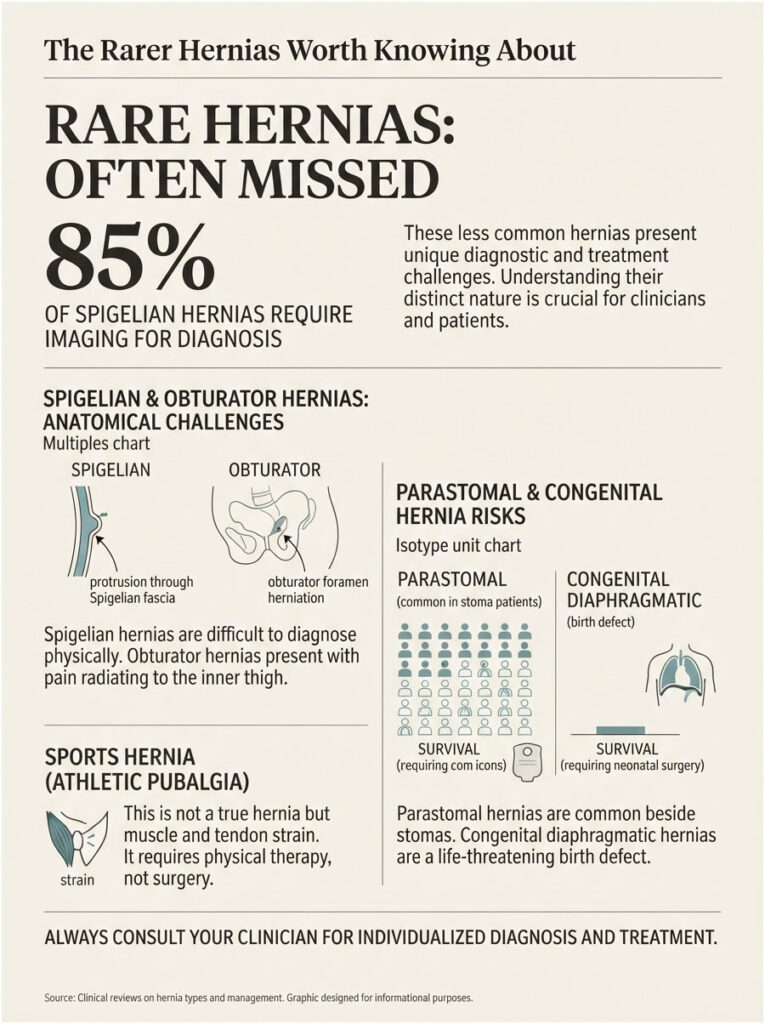
Obturator hernia passes through the obturator canal deep in the pelvis. It occurs almost entirely in thin, older women and typically presents as bowel obstruction with pain radiating down the inner thigh.
Parastomal hernia forms beside a colostomy or ileostomy. It is common in stoma patients and technically demanding to repair.
Congenital diaphragmatic hernia is a birth defect in which the diaphragm fails to close during development, allowing abdominal organs into the chest. It requires neonatal surgery.
Sports hernia (athletic pubalgia) is not a hernia at all. Nothing protrudes. It is a tear or strain of the muscles and tendons attaching to the pubic bone, common in hockey, soccer, and football players. First-line treatment is rest, anti-inflammatories, and physical therapy, not an operation.
How Hernias Are Diagnosed
Most hernias are found by a physician’s hands, not a machine.
The exam is straightforward. You stand, the physician places fingers over the suspected area, and asks you to cough or bear down. The bulge announces itself.
When imaging is needed
Ultrasound is first-line when the exam is unclear, and it is especially useful in women, where groin hernias are harder to feel and femoral hernias are easy to miss.
CT scan is the tool for complex, recurrent, and incisional hernias, and for anyone with obstruction symptoms. It maps the defect size and shows exactly what is inside the sac.
MRI offers higher sensitivity and specificity than ultrasound and is used to hunt occult hernias when clinical suspicion stays high despite a negative ultrasound.
How hiatal hernias are found
No external exam will reveal one. Diagnosis comes from upper endoscopy or a barium swallow, and both are often ordered when reflux fails to respond to medication.
The tests worth running before surgery
Before an elective repair, the surgical team will want a handful of numbers, and having them in hand speeds everything up.
Glucose control matters, because poor control raises wound infection and recurrence risk. Nicotine matters, because smoking impairs healing of the exact tissue being repaired.
Patients booking blood work with us often ask which panel to request. An HbA1c, a basic metabolic panel, a complete blood count, and a lipid profile cover most of what a surgical team wants to see.
The Mesh Question, Answered Honestly
Search “hernia mesh” and the first page of results is largely law firms. That is a poor information environment for a decision this consequential, so here is what the regulator’s own data actually says.
Why mesh became standard
Before mesh, surgeons pulled tissue together under tension. Tension pulls apart, and recurrence rates with older tension repairs ran as high as 15% at five years.
Mesh permits a tension-free repair. It cut recurrence sharply, which is why the large majority of hernia repairs in the United States now use it.
What the FDA data actually shows
FDA reviewed hernia mesh adverse event reports going back 22 years and found over 55,000 of them, roughly 60% linked to ventral or incisional repairs.
It also reviewed 45 published papers spanning 11 years, including nine randomized controlled trials, and published incidence ranges. Those ranges are wide because study definitions varied, but they are the most honest numbers publicly available.
| Complication | Reported Incidence Range | Source |
| Hernia recurrence | 0% to 11.1% | FDA literature review (45 studies) |
| Surgical site infection | 0% to 21% | FDA literature review |
| Mesh infection | 0% to 1.4% | FDA literature review |
| Seroma (fluid collection) | 0% to 52.5% | FDA literature review |
| Hematoma | 0.5% to 2.3% | FDA literature review |
| Bowel obstruction | Up to 3.8% | FDA literature review |
| Mesh bowel adhesion | Up to 3.2% | FDA literature review |
| Abdominal organ space infection | 0.22% to 1.1% | FDA literature review |
| Fistula formation | Under 1% | FDA literature review |
| Chronic pain (any definition) | 0.3% to 68% | FDA literature review |
| Chronic pain with major quality-of-life impact | Not exceeding 3.8% | FDA literature review |
Read the last two rows together, because they are the whole argument. The alarming 68% figure comes from studies counting any reported discomfort at any intensity. The number that actually matters, pain that meaningfully damages daily life, does not exceed 3.8%.
FDA also notes that many complications reported to it involved recalled mesh products that are no longer sold.
When mesh-free repair still makes sense
Small umbilical defects, pediatric repairs, Shouldice inguinal repairs in thin younger patients, and contaminated surgical fields where infection risk is elevated.
Ask about it. Do not assume the option is off the table.
What to ask your surgeon
FDA publishes a set of questions worth bringing to the consult. Paraphrased, they are worth saying out loud.
- What type of hernia do I have, precisely?
- What are my non-surgical and surgical options?
- Do you plan to use mesh, and what is it made of?
- Could this be repaired without mesh, and what would that trade off?
- What is my personal risk of recurrence, chronic pain, and infection?
- Afterward, can I have the manufacturer, brand name, and Unique Device Identifier of the mesh used?
That last question matters more than it sounds. If a safety notice ever touches your device, the identifier is how you will know it applies to you.
Open, Laparoscopic, or Robotic: How the Approaches Compare
The honest headline is that all three work, and the gaps between them are narrower than the marketing suggests.
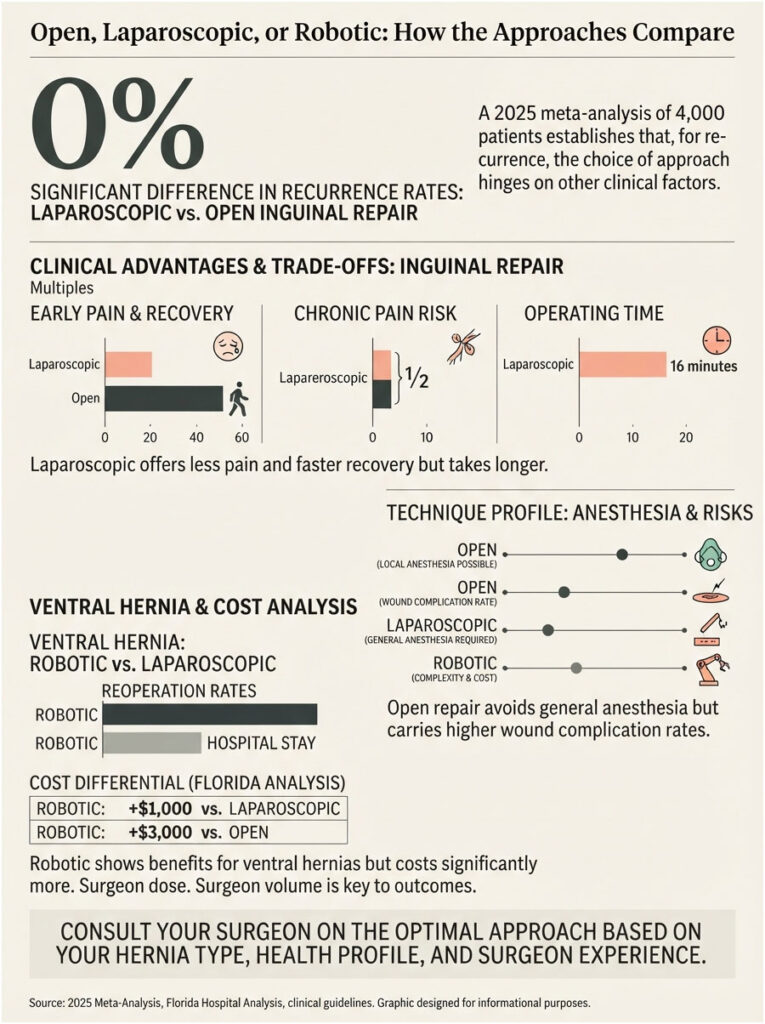
A 2025 meta-analysis of roughly 4,000 patients found no significant difference in recurrence between laparoscopic and open inguinal repair.
Where they genuinely differ
Laparoscopic repair produced less early postoperative pain, roughly half the odds of chronic groin pain, and a return to normal activity about a week earlier. It also ran about 16 minutes longer in the operating room and requires general anesthesia.
Open repair avoids general anesthesia, which is a real advantage for older or cardiopulmonary-compromised patients. Wound complications are more common with open repair, while serious deep abdominal complications are rarer.
What robotic actually buys you
For ventral and incisional hernias, robotic repair has shown lower reoperation rates and shorter hospital stays than standard laparoscopy.
For a straightforward one-sided inguinal hernia, the evidence for robotic superiority is thin. A Florida hospital analysis found robotic repairs cost at least $1,000 more than laparoscopic and about $3,000 more than open.
The variable that matters more than the technique
Surgeon volume. Our medical reviewers note that how many of your specific repair a surgeon performs each year predicts your outcome more reliably than which machine is in the room.
Ask the number out loud. A surgeon who does two hundred inguinal repairs a year is a different proposition from one who does twelve.
Wait or Operate? What the Evidence Says
This is the decision most readers came here to make.
The case for watching
For a small, painless inguinal hernia in a man, watchful waiting is a safe strategy. The risk of acute incarceration during observation is low, comfortably under 5%.
If serious heart or lung disease makes anesthesia genuinely risky, watching may be the better trade.
The case against waiting
Two facts belong side by side.
First, watching usually postpones surgery rather than replacing it. Seventy-two percent of watchful-waiting men still needed an operation within 7.5 years.
Second, if the hernia dictates the timing instead of you, the operation becomes far more dangerous. A nationwide analysis of 107,838 groin hernia repairs in the Swedish Hernia Register compared emergency with planned surgery, and the gap is not subtle.
| What the Number Describes | Figure | Source | Publication |
| 30-day mortality, emergency vs elective repair | 2.7% vs 0.1% | Swedish Hernia Register (107,838 repairs) | Journal of Clinical Medicine |
| 30-day complications, emergency vs elective | 21.9% vs 8.8% | Swedish Hernia Register | Journal of Clinical Medicine |
| Bowel resection required, emergency vs elective | 7.8% vs near zero | Swedish Hernia Register | Journal of Clinical Medicine |
| Chronic pain at 1 year, emergency vs elective | 20.6% vs 15.2% | Swedish Hernia Register | Journal of Clinical Medicine |
| Femoral hernias repaired as emergencies (women) | 41% | Swedish Hernia Register | Journal of Clinical Medicine |
| Crossover from watchful waiting to surgery by 7.5 years | 72% | Fitzgibbons et al. | Annals of Surgery |
| US inguinal hernia repairs per year | About 800,000 | StatPearls / NIH | NCBI Bookshelf |
| Lifetime risk of groin hernia (men / women) | 27% / 3% | American Family Physician | AAFP |
An elective hernia repair is among the safest operations in general surgery. The same repair, performed at 2 a.m. on a strangulated loop of bowel, is a different operation entirely.
Your Decision Guide
| Your Situation | What It Likely Means | Recommended Next Step | What to Ask For |
| Groin bulge, no pain, otherwise healthy man | Inguinal hernia, low urgency | Surgical consult within a few months | An honest discussion of watchful waiting vs elective repair |
| Groin bulge below the crease, especially in a woman | Possible femoral hernia | See a surgeon within weeks, not months | Ultrasound or CT, then prompt repair |
| A bulge you can no longer push back in, with pain | Incarcerated hernia | Same-day medical evaluation | Urgent imaging and surgical review |
| Bulge plus vomiting, fever, or red or dark skin | Possible strangulation | Emergency room now | Immediate surgical assessment |
| Navel bulge in a baby under 4 | Infant umbilical hernia | Routine pediatric follow-up | Reassurance and observation, not surgery |
| Navel bulge in an adult | Adult umbilical hernia | Surgical consult | Mesh vs suture repair discussion |
| Bulge through an old surgical scar | Incisional hernia | Surgical consult; repair before it grows | CT to map the defect; optimize weight and HbA1c first |
| Heartburn and regurgitation, no visible bulge | Possible hiatal hernia | Gastroenterology referral | Upper endoscopy; ask which hiatal type it is |
| Chest pain, trouble swallowing, early fullness | Possible paraesophageal hernia | Prompt specialist evaluation | Imaging; Types II to IV usually need repair |
Recovery: What the First Six Weeks Actually Look Like
Recovery is the question people ask their surgeon last and Google first. Here is the realistic version.
| Repair Type | Back to Desk Work | Back to Driving | Back to Heavy Lifting | Full Recovery |
| Laparoscopic inguinal | 1 to 2 weeks | 3 to 7 days | 3 to 4 weeks | 3 to 4 weeks |
| Open inguinal | 2 to 3 weeks | 1 to 2 weeks | 4 to 6 weeks | 4 to 6 weeks |
| Umbilical (small, adult) | 1 to 2 weeks | 3 to 7 days | 3 to 4 weeks | 3 to 4 weeks |
| Laparoscopic or robotic ventral | 2 to 3 weeks | 1 to 2 weeks | 4 to 6 weeks | 4 to 6 weeks |
| Open incisional (complex) | 3 to 6 weeks | 2 to 3 weeks | 6 to 8 weeks | 8 to 12 weeks |
| Hiatal with fundoplication | 2 to 3 weeks | 1 to 2 weeks | 4 to 6 weeks | 6 weeks, plus a staged diet |
Week one
Expect soreness, bruising, and swelling. Swelling around a groin repair can look alarming and is usually normal.
Walk from day one. Short, frequent walks reduce clot risk and speed the return of bowel function. Do not lie in bed for a week.
Weeks two to four
Most desk workers are back. Pain shifts from constant to intermittent, and most people are off prescription pain medication within a week.
Stay ahead of constipation. Straining on the toilet applies exactly the pressure the repair is trying to resist.
Weeks four to six
Lifting restrictions lift, in stages. Manual workers, athletes, and anyone whose job involves carrying will typically be cleared at the six-week mark.
If you had a fundoplication, your diet advances in stages from liquids to soft foods to solids across several weeks.
Lifting restrictions are not arbitrary
The repair holds while your own tissue grows into and around it. Load it too early and the repair can fail before that integration is complete.
Recurrence after an early return to heavy lifting is not bad luck. It is physics.
How to Keep It From Coming Back
Four modifiable factors do most of the work, and all four are measurable before surgery.
Smoking. Nicotine impairs the healing of connective tissue, which is precisely what a hernia repair depends on. Stopping four to six weeks before surgery meaningfully improves outcomes.
Blood sugar. Poor glucose control raises wound infection and recurrence risk. An HbA1c is the number your surgical team will want.
Weight. Excess abdominal weight applies constant pressure to the repair. For incisional and umbilical hernias in particular, weight loss before surgery reduces recurrence.
Chronic straining. Untreated constipation, chronic cough, and prostate-related straining all push on the repair every single day. Treat them before the operation, not after.
Our lab partners report that pre-surgical panels are the step patients skip most often and regret most often. The measurement takes a day. The recurrence takes another operation.
What Hernia Repair Costs in the US
Hernia repair averages around $7,750 at a hospital outpatient department, with bills commonly landing between $3,500 and $15,000.
The facility is the biggest lever
Hospital outpatient departments charge roughly 8.3 times the Medicare rate on average. Ambulatory surgery centers average about 4.1 times.
For the identical procedure code, that gap can be $3,000 to $5,000 out of your pocket. Ask whether an in-network ambulatory surgery center is an option, because for a routine repair, it usually is.
Insurance
Medicare, Medicaid, Tricare, and most private plans cover hernia repair as medically necessary. Your share depends on your deductible, coinsurance, and facility choice.
Get the CPT code, get the estimate in writing, and get it before you schedule.
Red Flags: Go to the ER Tonight
Do not wait for a clinic appointment if any of these appear.
- A hernia bulge you can no longer push back in
- Sudden, severe pain at the hernia site
- Skin over the bulge turning red, purple, or dark
- Nausea, vomiting, or an inability to pass gas or stool
- Fever alongside abdominal pain
- A firm, tender lump that was soft and painless yesterday
Strangulated tissue starts dying within hours. Time from onset to surgery is the strongest single predictor of the outcome.
Frequently Asked Questions
What are the 7 main types of hernias?
Inguinal (groin, above the crease), femoral (groin, below the crease), umbilical (navel), incisional (through a surgical scar), ventral or epigastric (abdominal midline), hiatal (stomach through the diaphragm), and a rare group including Spigelian, obturator, parastomal, and congenital diaphragmatic hernias.
Which type of hernia is the most dangerous?
Femoral hernias, among the common types. The femoral canal has rigid walls, so trapped tissue cannot slide back out, and roughly 30% present as an emergency. Paraesophageal hiatal hernias (Types II to IV) are the other high-risk group, because the stomach can twist or become trapped.
Can a hernia heal on its own without surgery?
In adults, no. Fascia has no mechanism to close a defect under constant abdominal pressure, so hernias enlarge rather than shrink. The one genuine exception is infant umbilical hernias, roughly 85% of which close on their own by age five with no intervention at all.
What happens if you leave a hernia untreated?
It usually enlarges and becomes more symptomatic. The serious risk is incarceration, then strangulation, where trapped tissue loses its blood supply. Emergency repair carries a 30-day mortality of 2.7% against 0.1% for planned surgery, and 7.8% of emergency cases require bowel resection.
How do I know what type of hernia I have?
Location does most of the work. Above the groin crease points to inguinal, below it to femoral, at the navel to umbilical, through a scar to incisional. Heartburn with no visible bulge suggests hiatal. A physical exam confirms it, with ultrasound or CT when the exam is unclear.
Is hernia mesh safe?
For most people, yes. FDA’s literature review found recurrence ranging from 0% to 11.1% and mesh infection from 0% to 1.4%. Chronic pain with significant impact on quality of life did not exceed 3.8%. Many complications reported to FDA involved recalled products no longer on the market.
How long is recovery from hernia surgery?
Laparoscopic repair typically means one to two weeks before desk work and three to four weeks before heavy lifting. Open repair runs two to three weeks and four to six weeks respectively. Complex incisional repairs can take eight to twelve weeks for full recovery.
Is laparoscopic hernia repair better than open?
Not universally. A 2025 meta-analysis of roughly 4,000 patients found no difference in recurrence. Laparoscopic repair produced less early pain, about half the odds of chronic groin pain, and return to activity a week sooner, but it needs general anesthesia and slightly longer operating time.
Do umbilical hernias in babies always need surgery?
No. Up to 25% of newborns have one, and about 85% close on their own by age five. Complications are rare, with incarceration estimated at 0.2% to 4.5%. Surgery is generally reserved for hernias that persist past age four or five, exceed about 1.5 cm, or become symptomatic.
How much does hernia surgery cost in the US?
Bills average around $7,750 at hospital outpatient departments, with a common range of $3,500 to $15,000. Facility choice is the biggest variable, since ambulatory surgery centers charge dramatically less than hospitals for the same procedure code, often a $3,000 to $5,000 difference.
Can you push a hernia back in yourself?
A reducible hernia often slides back with gentle pressure while lying down, and that is not dangerous. Never force it. If a hernia suddenly refuses to reduce, or forcing it produces sharp pain, stop immediately and seek care, because that is how incarceration announces itself.
Can you exercise or lift weights with a hernia?
Light activity and cardiovascular exercise are generally fine. Heavy lifting, straining, and maximal core work raise abdominal pressure and can enlarge the defect. Ask your surgeon for specific limits. A truss or binder may ease symptoms temporarily but it repairs nothing.
Medical Disclaimer: This article is for general education and is not medical advice, diagnosis, or treatment. HealthCareOnTime does not perform surgery or prescribe treatment. Hernia management depends on type, size, symptoms, and your individual health, and should be decided with a qualified surgeon. Seek emergency care immediately for a hernia bulge that cannot be pushed back in, sudden severe pain, discolored skin over the bulge, vomiting, or fever.
References
- FDA, Surgical Mesh for Hernia Repair: FDA Activities
- FDA, Surgical Mesh Used for Hernia Repair: Information for Patients
- American Family Physician, Inguinal Hernias: Diagnosis and Management
- AAFP Choosing Wisely, Umbilical Hernias in Children
- NIH StatPearls, Inguinal Hernia
- NIH StatPearls, Minimally Invasive Inguinal Hernia Repair
- NIH StatPearls, Pediatric Umbilical Hernia
- Journal of Clinical Medicine, Outcomes After Emergency Groin Hernia Surgery (Swedish Hernia Register)
- Annals of Surgery, Long-Term Results of Watchful Waiting for Minimally Symptomatic Inguinal Hernias
- BMC Surgery, Meta-Analysis Comparing Laparoscopic and Open Inguinal Hernia Repair
- Cleveland Clinic, Hernia: Types, Causes, and Treatment
- Columbia Surgery, Hernia Types, Causes, and Treatments
- UCSF Department of Surgery, Inguinal Hernia
- Foregut Surgery review, Hiatal Hernia: Key Principles
- Health Care Cost Institute data via BillKarma, Hernia Surgery Cost Guide





