The side effect that drives most people off Zepbound is almost never the one printed in the boxed warning. It’s a Tuesday morning, four days after a dose increase, when the nausea won’t quit and the pen sitting in the refrigerator door starts to look like a mistake.
Table of Contents
Here is the number that reframes everything. Gastrointestinal reactions hit 56% of patients on Zepbound in the pivotal trials, against 30% on placebo. Yet only 4.8% to 6.7% of patients actually stopped the drug because of side effects.
That gap, between “almost everyone feels something” and “almost nobody quits over it,” is where the useful information lives. This article is built to close it.
Quick Answer
The most common Zepbound side effects are nausea (25% to 29%), diarrhea (19% to 23%), constipation (11% to 17%), and vomiting (8% to 13%), per the FDA label. They cluster in the first four weeks and after each dose increase, then fade. Most are mild. Serious events like pancreatitis, gallbladder disease, and kidney injury are uncommon. Roughly 5% to 7% of users stop treatment because of side effects.
At a Glance
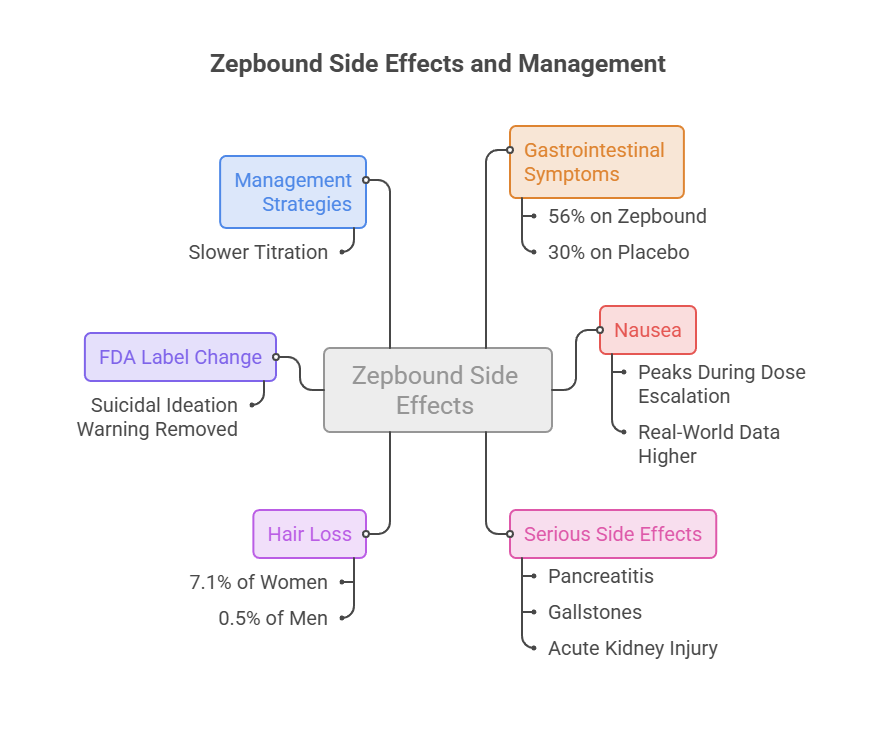
- Gastrointestinal symptoms are the rule, not the exception: 56% on Zepbound versus 30% on placebo.
- Nausea is the single most reported symptom, and it peaks during dose escalation, not at steady state.
- Real-world survey data run higher than trial data, with about half of GLP-1 users reporting nausea.
- Serious Zepbound side effects (pancreatitis, gallstones, acute kidney injury) sit at or below 1% to 2% in trials.
- Hair loss shows a sharp sex split: 7.1% of women versus 0.5% of men.
- The FDA label changed in early 2026, and the suicidal ideation warning was removed.
- Slower titration is the strongest lever you have over how bad any of this feels.
What Zepbound Actually Does Inside You (and Why That Causes Side Effects)
Zepbound is tirzepatide, and it is not a plain GLP-1 drug. It switches on two gut hormone receptors at once, GIP and GLP-1, both of which live in brain regions that regulate appetite and food intake.
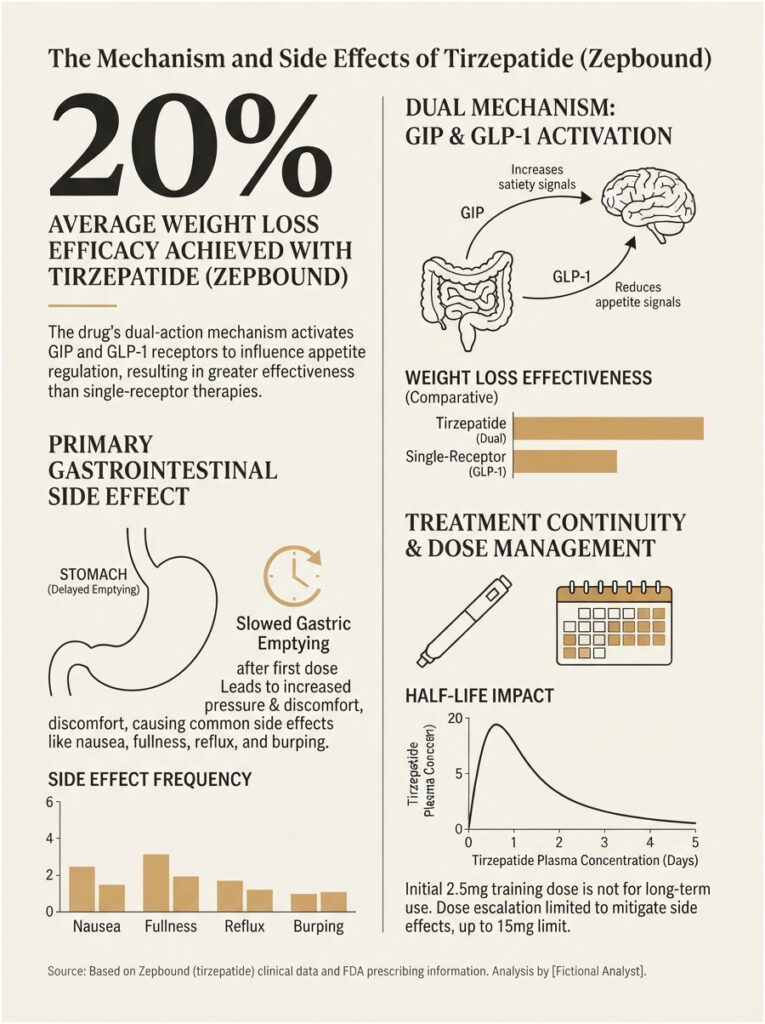
That dual action is why it outperforms single-receptor drugs on weight. It is also why the stomach files a complaint.
Delayed Gastric Emptying, the Root of Most Complaints
Tirzepatide slows how fast the stomach empties, and that delay is largest after the very first dose before diminishing over time. Food sits longer. Pressure builds. Nausea, fullness, reflux, and burping follow from plain mechanics.
Patients booking metabolic panels through HealthCareOnTime ask this constantly: why does a weight-loss injection wreck digestion? Nothing mysterious is happening. The drug is doing precisely what it was designed to do, and the discomfort shares a single mechanism with the appetite suppression people are paying for.
Why 2.5 mg Is a Training Dose, Not a Treatment Dose
The label starts everyone at 2.5 mg once weekly for four weeks, then permits increases in 2.5 mg steps no sooner than every four weeks, to a ceiling of 15 mg. The 2.5 mg dose exists for initiation and is not approved as a maintenance dose.
The FDA says outright that this escalation schedule exists to reduce the risk of gastrointestinal adverse reactions. The ladder is a side effect tool, not a bureaucratic formality.
Tirzepatide has an elimination half-life of roughly five to six days. That is why a bad week does not resolve overnight, and why a missed dose can never simply be doubled up later.
The Most Common Zepbound Side Effects, By the Numbers
Most articles online flatten this into “up to 29%.” The actual FDA table breaks every symptom out by dose against placebo, and the pattern it reveals is more useful than any summary anyone has written about it.
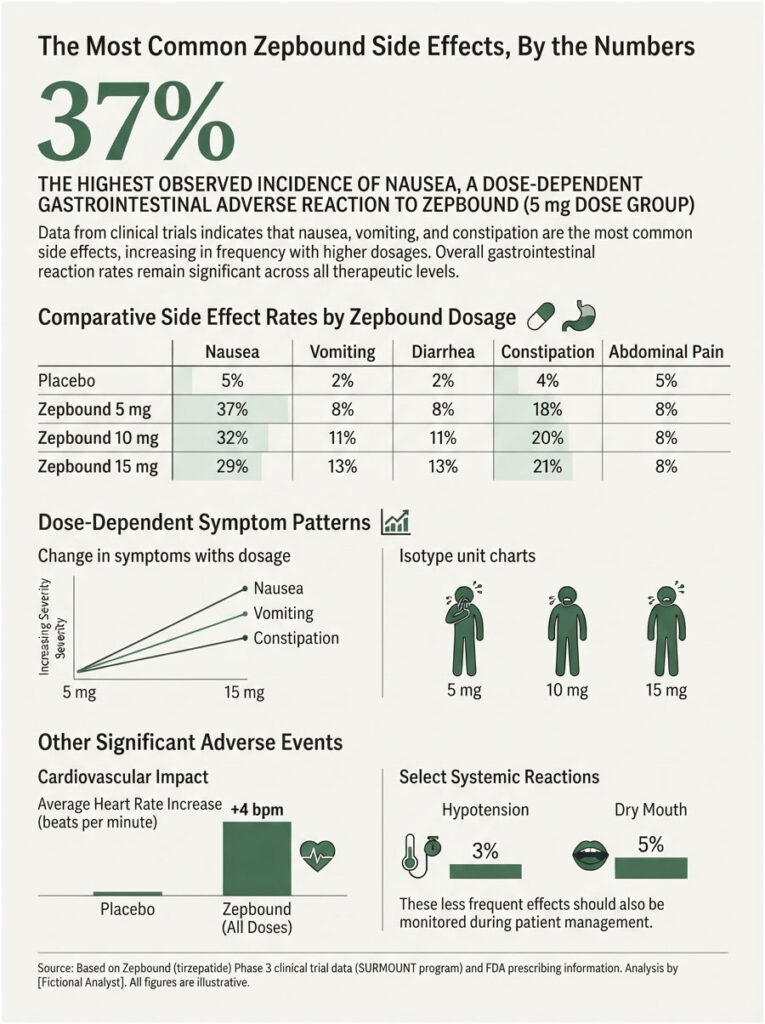
Table 1: Zepbound Side Effects by Dose vs Placebo
Pooled data from the two placebo-controlled weight-reduction trials (2,519 adults treated for up to 72 weeks), reported in the prescribing information revised February 2026.
| Adverse Reaction | Placebo (n=958) | Zepbound 5 mg (n=630) | Zepbound 10 mg (n=948) | Zepbound 15 mg (n=941) |
| Nausea | 8% | 25% | 29% | 28% |
| Diarrhea | 8% | 19% | 21% | 23% |
| Vomiting | 2% | 8% | 11% | 13% |
| Constipation | 5% | 17% | 14% | 11% |
| Abdominal pain | 5% | 9% | 9% | 10% |
| Dyspepsia (indigestion) | 4% | 9% | 9% | 10% |
| Injection site reactions | 2% | 6% | 8% | 8% |
| Fatigue | 3% | 5% | 6% | 7% |
| Hypersensitivity reactions | 3% | 5% | 5% | 5% |
| Eructation (burping) | 1% | 4% | 5% | 5% |
| Hair loss | 1% | 5% | 4% | 5% |
| Acid reflux (GERD) | 2% | 4% | 4% | 5% |
| Flatulence | 2% | 3% | 3% | 4% |
| Abdominal distension | 2% | 3% | 3% | 4% |
| Dizziness | 2% | 4% | 5% | 4% |
| Hypotension | 0% | 1% | 1% | 2% |
Source: FDA Zepbound Prescribing Information, revised February 2026
What the Table Actually Tells You
Look at the vomiting row. It climbs with dose, 8% to 11% to 13%. Now look at constipation. It runs the other way, 17% down to 11%. Dose is not a simple volume knob on misery. It reshapes which symptom you get.
Then look at the number that isn’t in the table. Overall gastrointestinal reactions ran 56% at 5 mg, 56% at 10 mg, and 56% at 15 mg alike, against 30% on placebo. Parking yourself at a low dose forever does not buy a clean stomach. It buys a different mix of symptoms and less weight loss.
The Label Entries Nobody Talks About
Hypotension occurred in 1.6% of Zepbound patients versus 0.1% on placebo, and it was more frequent in patients already on blood pressure medication (2.2%) than in those who were not (1.2%). Dry mouth was reported by 1% of patients and dysgeusia, a distorted sense of taste, by 0.4%.
Heart rate rose by an average of one to three beats per minute. Small on paper. Occasionally alarming when a patient spots it on a smartwatch and assumes the worst.
Trial Numbers vs Real Life: Why Your Experience May Be Rougher
Clinical trials recruit motivated people who get coached, monitored, and phoned. Real life does not phone you. When the RAND Corporation surveyed a nationally representative panel of US adults, the reported side effect rates came in far above the trial figures.
Table 2: Clinical Trial Rates vs Real-World Reported Rates
| Metric | Clinical Trial Rate | Real-World Rate | Source |
| Nausea | 28% (15 mg) | 52.0% (43.2% mild, 8.8% serious) | FDA label 02/2026; RAND American Life Panel 2025, n=1,262 GLP-1 users |
| Diarrhea | 23% (15 mg) | 34.3% (26.8% mild, 7.5% serious) | FDA label 02/2026; RAND 2025 |
| Vomiting | 13% (15 mg) | 19.8% (14.4% mild, 5.4% serious) | FDA label 02/2026; RAND 2025 |
| Facial volume loss | Not tracked | 8.5% (7.4% mild, 1.1% serious) | RAND 2025 |
| Stopped within 3 months | 4.8% to 6.7% (all reasons) | 16.4% of tirzepatide users | FDA label 02/2026; Cleveland Clinic cohort, Obesity 2025, n=7,881 |
| Weight loss at 1 year | 20.9% (15 mg, 72 weeks) | 12.4% | SURMOUNT-1 (NEJM); Cleveland Clinic 2025 |
The RAND Finding, and What It Does Not Mean
Among 1,262 US adults who had taken a GLP-1, 52.0% reported nausea, 34.3% reported diarrhea, and 19.8% reported vomiting. The majority described these symptoms as mild rather than serious.
That last clause carries the weight. Only 8.8% rated their nausea as serious. Only 7.5% said the same of diarrhea. The volume of complaints is high. The severity of complaints is mostly low.
Our medical reviewers note that surveys and trials measure different things. A trial logs what an investigator classifies as an adverse event. A survey logs what a person remembers about a bad week eight months ago. Both are honest. Neither is the whole picture.
The national backdrop explains the urgency. A KFF Health Tracking Poll found 12% of US adults are currently taking a GLP-1 drug, and among those who stopped, 13% named side effects as the reason.
The Zepbound Side Effect Timeline: When It Starts and When It Fades
The most-searched question about this drug is how long Zepbound side effects last. The honest answer is that they are not one continuous event. They arrive in waves, and the waves are scheduled by your dose ladder.
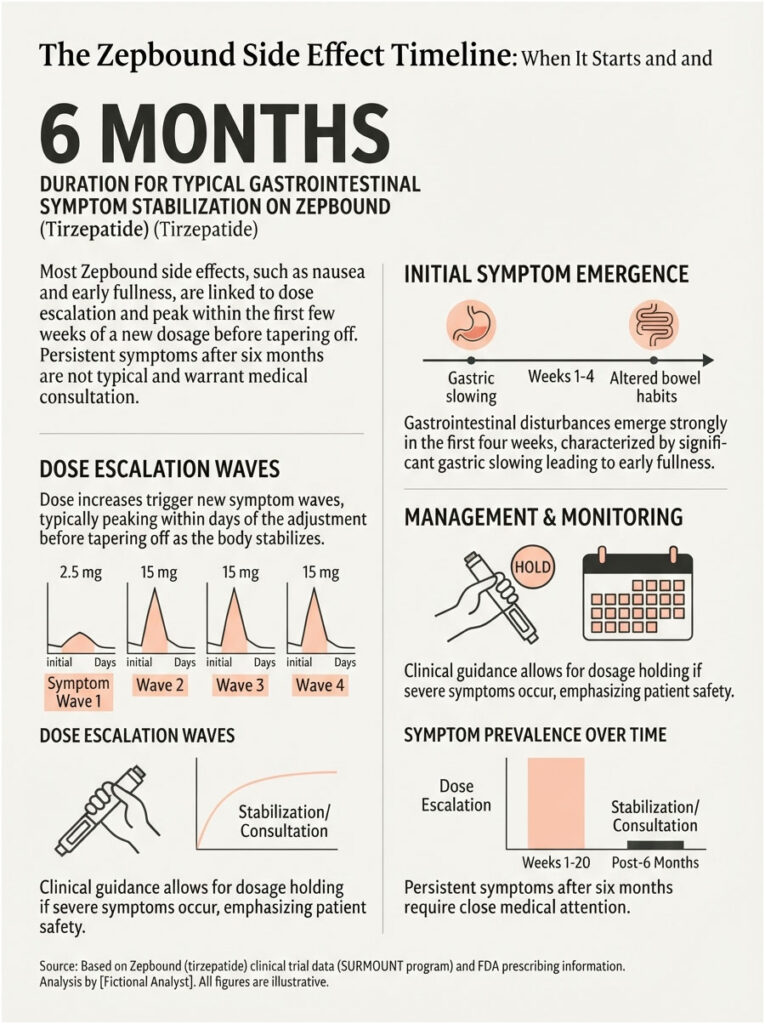
Weeks 1 to 4: The Starter Phase
Your first injection produces the strongest slowdown in gastric emptying you will ever experience on this drug. Expect early fullness, mild queasiness, and a swing toward either loose stools or constipation.
Pooled analysis across the SURMOUNT-1 through SURMOUNT-4 trials confirmed that gastrointestinal events were reported primarily during dose escalations. Weeks one through four are your first escalation, even though nothing has been increased yet.
Weeks 5 to 20: The Escalation Waves
Every 2.5 mg step restarts the adjustment clock. Symptoms typically flare within 24 to 72 hours of the new dose and settle over the following several days.
Patients commonly tell us the second and third increases feel worse than the first. That is normal. The body is adapting to a higher exposure, not failing to adapt.
What a Dose-Increase Wave Feels Like
Day one, nothing unusual. Days two through four, appetite collapses, food tastes wrong, nausea shows up after meals. Days five through seven, it lifts. Then you plateau until the next step up.
If a wave never lifts, that is your signal to call about holding the dose rather than climbing. Holding is a legitimate clinical decision, and the label explicitly permits a lower maintenance dosage for patients who do not tolerate a higher one.
Maintenance: Why Symptoms Usually Settle
The FDA notes that the majority of nausea, vomiting, and diarrhea events occurred during dose escalation and decreased over time. Once you stop climbing, most people find the gut recalibrates within a few weeks.
If Symptoms Return at Month Six
New or worsening digestive symptoms long after you reach a stable dose are not typical, and they should not be shrugged off as “just the Zepbound.” Postmarketing reports for tirzepatide include ileus, intestinal obstruction, and severe constipation with fecal impaction.
That combination, no bowel movement plus bloating plus vomiting, is not a titration wave. It is a phone call.
Serious Zepbound Side Effects: Which Need a Call, Which Need 911
Nine safety warnings sit in the current label. Here is what each one means for a person actually holding the pen.
The Boxed Warning: Thyroid C-Cell Tumors
In rats, tirzepatide caused dose-dependent and duration-dependent thyroid C-cell tumors. Whether it causes these tumors in humans, including medullary thyroid carcinoma, is unknown, because the human relevance of the rodent finding has not been determined.
Zepbound is contraindicated if you or a family member has had medullary thyroid carcinoma, or if you have Multiple Endocrine Neoplasia syndrome type 2. Routine calcitonin testing or thyroid ultrasound is of uncertain value for early detection and may drive unnecessary procedures.
Our medical team’s position is simple. This is a warning to screen against before you start, not a symptom to monitor for after you start.
Acute Pancreatitis
In the pooled weight-reduction trials, adjudicated acute pancreatitis occurred in 0.2% of Zepbound patients and 0.2% of placebo patients. The rates matched, which argues against a strong signal at trial scale.
The symptom to watch is severe, persistent abdominal pain that may radiate to the back, with or without vomiting. Stop the drug and get evaluated.
Gallbladder Disease
Gallstones were reported in 1.1% of Zepbound patients versus 1% on placebo, gallbladder inflammation in 0.7% versus 0.2%, and gallbladder removal in 0.2% versus none. These events were associated with the weight reduction itself, which is a known trigger for gallstone formation at any speed.
Acute Kidney Injury
Acute kidney injury was reported in 0.5% of Zepbound patients versus 0.2% on placebo, and most postmarketing cases followed dehydration from nausea, vomiting, or diarrhea, with some requiring dialysis.
The kidney risk sits downstream of the gut risk. That is why hydration is not filler advice. It is the intervention.
Hypoglycemia
In the type 2 diabetes trial, blood sugar below 54 mg/dL occurred in 4.2% of Zepbound patients versus 1.3% on placebo. Among Zepbound patients also taking a sulfonylurea, that rate jumped to 10.3%, against 2.1% for those not taking one.
If you take insulin or a sulfonylurea, your prescriber should be talking about lowering those doses when Zepbound starts.
Severe Allergic Reactions and Anesthesia Risk
Severe hypersensitivity reactions occurred in 0.1% of Zepbound patients and in no placebo patients, with postmarketing reports of anaphylaxis and angioedema.
There have also been rare reports of pulmonary aspiration in patients on GLP-1 drugs undergoing procedures requiring general anesthesia or deep sedation, some of whom had food still in the stomach despite following fasting instructions.
Table 3: What To Do, Symptom by Symptom
| What You’re Feeling | Likely Cause | Urgency | Recommended Action |
| Mild nausea 2 to 4 days after a dose increase | Expected titration response | Manage at home | Small low-fat meals, steady fluids, stay upright after eating. Track it. |
| Vomiting past 24 hours, cannot keep fluids down | Severe GI reaction, dehydration risk | Call your prescriber today | Ask about holding the dose. Push electrolytes. Watch urine output. |
| Severe stomach pain radiating to the back | Possible acute pancreatitis | Emergency care now | Stop Zepbound. Go to the ER. Do not restart without clearance. |
| Right upper belly pain, fever, yellow eyes, pale stools | Possible gallbladder disease | Emergency care now | ER evaluation. Gallbladder imaging is indicated. |
| Barely urinating, dizzy on standing, very dry mouth | Dehydration, possible kidney injury | Call today, ER if worsening | Rehydrate. Request kidney function testing. |
| Shakiness, sweating, confusion (on insulin or sulfonylurea) | Hypoglycemia | Treat now, then call | 15 g fast-acting carbs, recheck in 15 minutes. Below 55 mg/dL, get help. |
| Lump in the neck, hoarseness, trouble swallowing | Thyroid warning symptom | Call your prescriber promptly | Report it. Do not self-order calcitonin testing. |
| Face, lip, tongue, or throat swelling, trouble breathing | Anaphylaxis or angioedema | Call 911 | Stop Zepbound permanently. Emergency treatment. |
| No bowel movement, bloating, vomiting | Possible ileus or obstruction | Emergency care now | Do not take laxatives blindly. Get imaging. |
| Surgery, colonoscopy, or sedation scheduled | Pulmonary aspiration risk | Call before the procedure | Tell every provider you take Zepbound. It delays gastric emptying. |
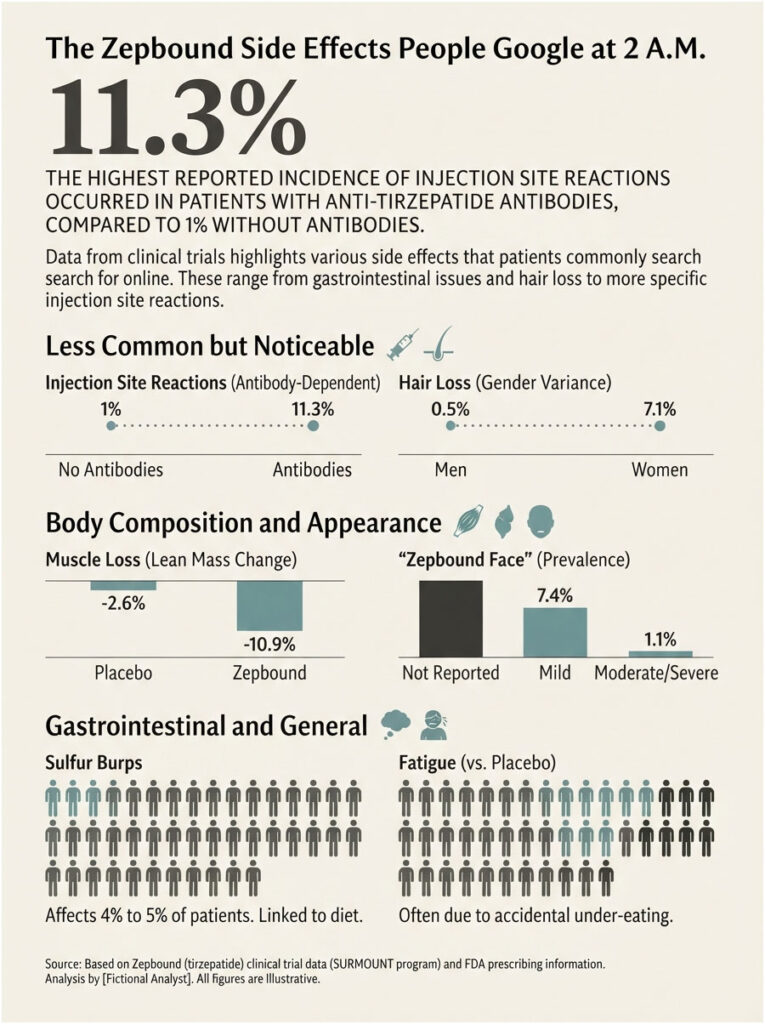
The Zepbound Side Effects People Google at 2 A.M.
Sulfur Burps
The label calls it eructation. It affected 4% to 5% of patients versus 1% on placebo. Slowed stomach emptying means protein-rich food ferments longer, gut bacteria go to work on it, and hydrogen sulfide gas comes back up.
Practical fixes: cut high-sulfur foods (eggs, red meat, broccoli, garlic) in the two or three days after your injection, shrink portions, skip carbonation, and stop chewing gum, which pulls air into the stomach.
Hair Loss and the 7.1% vs 0.5% Split
This is the number no competing article reports. Hair loss was reported in 7.1% of women on Zepbound versus 0.5% of men, compared with 1.3% of women on placebo.
The FDA links these events to weight reduction rather than to a direct drug effect, and no Zepbound patient in the trials discontinued because of it. The pattern is telogen effluvium, the diffuse shedding that follows rapid weight change, and it typically resolves.
Across the patients we serve, hair shedding is the complaint most likely to arrive without warning, usually around month three or four, well after the nausea has faded and the person assumed they were in the clear. It is also the complaint most likely to be a nutrient story rather than a drug story, which is why iron, ferritin, and vitamin B12 belong in the workup.
“Zepbound Face”
In the RAND survey, 8.5% of GLP-1 users reported a hollowed-out face, and 7.4% called it mild. There is no special drug mechanism at work. Facial fat is fat, and it leaves along with the rest.
Muscle Loss: What the DXA Scans Actually Showed
The body composition substudy inside SURMOUNT-1 scanned 160 participants with DXA at baseline and week 72. Body weight fell 21.3%, fat mass fell 33.9%, and lean mass fell 10.9% on tirzepatide, against 5.3%, 8.2%, and 2.6% on placebo.
Roughly 75% of the weight lost was fat and 25% was lean mass, and that ratio was identical in the tirzepatide and placebo groups. Participants also reported improved physical function scores despite the drop in lean mass.
Read that carefully. Zepbound does not strip muscle faster than ordinary weight loss does. It produces far more weight loss, so the absolute muscle number is bigger. The ratio is normal. The scale is not.
Fatigue That Won’t Lift
Fatigue was reported by 5% to 7% of patients versus 3% on placebo. The usual culprit is accidental under-eating. When appetite vanishes, people fall into a calorie and protein deficit they never consciously chose.
Injection Site Reactions and the Antibody Link
Anti-tirzepatide antibodies were detected in 64.5% of treated patients. Among those with antibodies, injection site reactions occurred in 11.3%, against 1% in those without them. No clinically meaningful effect of these antibodies on how well Zepbound works has been identified.
What Changed on the Zepbound Label in 2026
Most Zepbound side effect articles online still cite a 2024 version of the prescribing information. Three things have changed since, and all three matter.
The Suicidal Ideation Warning Was Removed
On January 13, 2026, the FDA requested that manufacturers remove the suicidal ideation and behavior warning from the labeling of Saxenda, Wegovy, and Zepbound, after a review found no increased risk.
The agency’s analysis pooled 91 placebo-controlled trials covering 107,910 patients, 60,338 on GLP-1 drugs and 47,572 on placebo, and found no increased psychiatric risk. The label revised in February 2026 lists that warning as removed.
The FDA still advises clinicians to discuss the findings with patients and to refer anyone reporting suicidal thoughts to mental health professionals. Removing a label warning is not the same as dismissing a person’s experience.
A Pen-Sharing Warning Was Added
The label now carries a dedicated warning never to share a Zepbound KwikPen between patients, even with a new needle, because of blood-borne pathogen transmission risk.
Compounded Tirzepatide Is a Different Risk Category
The FDA has received adverse event reports tied to dosing errors with compounded semaglutide and tirzepatide, some requiring hospitalization, largely from patients drawing and self-administering incorrect doses from vials.
Through the end of 2024, the FDA’s adverse event database logged more than 900 cases linked to compounded versions of these drugs, including 17 deaths. If you are researching Zepbound side effects while taking a compounded product, you are reading the wrong safety data.
Zepbound vs Wegovy: Which Is Easier on the Stomach?
SURMOUNT-5 put them head to head in 751 US adults across 32 sites over 72 weeks. It is the only direct comparison that exists.
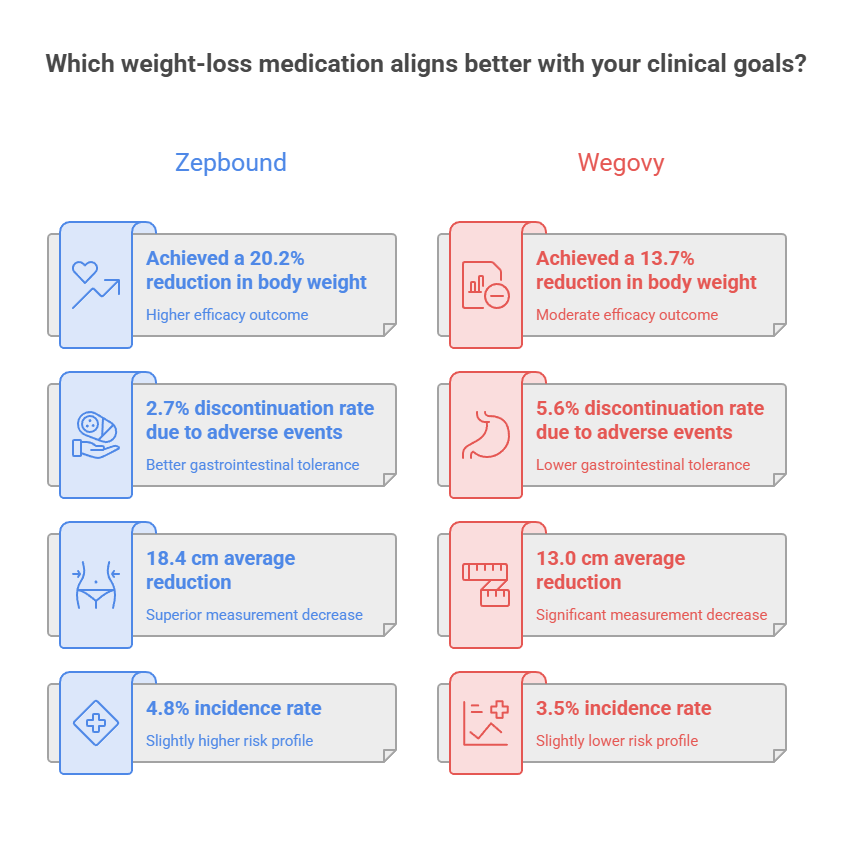
Tirzepatide produced 20.2% mean weight loss against 13.7% for semaglutide, and waist circumference fell 18.4 cm against 13.0 cm.
On tolerability, the result surprises nearly everyone. Gastrointestinal adverse events causing discontinuation were more frequent with semaglutide (5.6%) than with tirzepatide (2.7%).
Serious adverse events ran slightly higher on tirzepatide (4.8%) than semaglutide (3.5%), with six patients in each group leaving the trial because of adverse events.
More weight loss did not translate into more people quitting over their gut. The intuitive tradeoff, that harder-hitting means harder to tolerate, did not hold.
None of which tells you anything about you. A population average cannot predict an individual response, some people tolerate one of these drugs and not the other, and no test exists that forecasts which one you are.
How to Cut Your Side Effect Risk Without Quitting
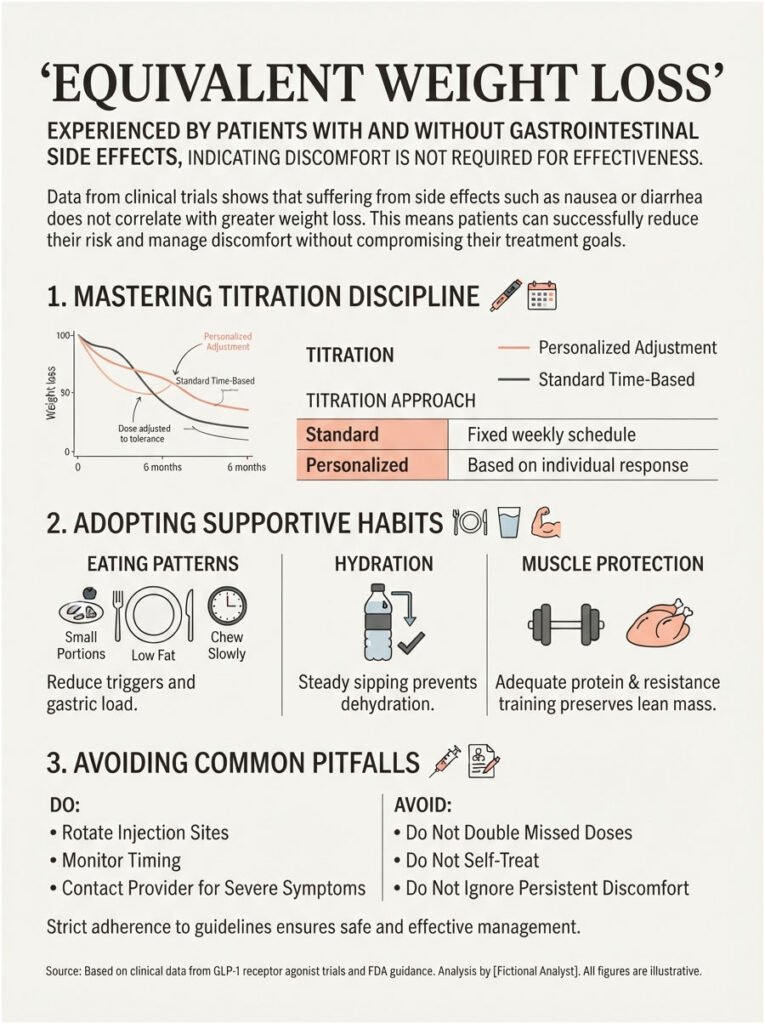
Titration Discipline Is the Biggest Lever You Have
The label permits a dose increase after at least four weeks. Not exactly four weeks. If a step is going badly, staying put is a clinical option the FDA explicitly endorses.
There is also a finding buried in the trial data that should change how you think about all of this: weight loss was nearly the same in patients who experienced gastrointestinal side effects and in those who did not.
Suffering is not the mechanism. You do not have to feel sick for Zepbound to work.
Eating Patterns That Actually Help
Small volumes, low fat, slow chewing. Fried and greasy food is the most reliable trigger when the stomach is already emptying at half speed.
Stop at the first sense of fullness rather than at the bottom of the plate. Your satiety signal now arrives earlier than your habits expect it to.
Hydration and Electrolytes
Dehydration is the bridge between a manageable side effect and a hospital admission. Steady sipping through the day beats large volumes at once, which only worsens fullness.
Protect Lean Mass on Purpose
Adequate protein plus resistance training two or three times weekly is the standard defense for anyone losing weight this fast. The DXA data shows the fat-to-lean ratio is normal, but the absolute muscle loss still deserves an active response.
Timing and Technique
Rotate injection sites with every dose. Some people find injecting on a Friday gives them the weekend to absorb the worst of a dose-increase wave.
If you miss a dose, take it within four days (96 hours). Beyond that, skip it and resume your regular schedule. Never take two doses within 72 hours of each other.
In cases reviewed by our medical team, the patients who struggle most are rarely the ones with the worst symptoms. They are the ones who pushed to 15 mg on a fixed schedule because they thought a slower ladder meant failure, and then quit entirely eight weeks later.
What Not To Do
Do not double a missed dose. Do not push through vomiting that has stopped you from drinking. Do not self-treat suspected pancreatitis with antacids and hope. Do not stop your own insulin or sulfonylurea without a prescriber.
Interactions and Situations That Change the Risk Math
Oral Birth Control: the Four-Week Rule
This one gets missed constantly. Zepbound can reduce the effectiveness of oral hormonal contraceptives because of delayed gastric emptying.
The FDA advises switching to a non-oral method, or adding a barrier method, for four weeks after starting Zepbound and for four weeks after every single dose escalation. Non-oral hormonal contraceptives are not affected.
Do the arithmetic on a 20-week escalation. That is five or six separate windows of reduced protection, not one.
Insulin and Sulfonylureas
Consider reducing the dose of insulin or an insulin secretagogue when starting Zepbound, because the hypoglycemia risk multiplies in combination. This is a prescriber decision, not a self-adjustment.
Other Oral Medications
Zepbound delays gastric emptying and can affect the absorption of oral drugs. The label singles out medications with a narrow therapeutic index, such as warfarin, for monitoring.
Alcohol
No formal contraindication exists, but alcohol irritates the stomach lining, dehydrates, and lowers blood pressure. On a drug that already slows gastric emptying and was linked to hypotension in 1.6% of patients, it stacks badly. Nausea, dizziness, and reflux all get louder.
Surgery, Colonoscopy, and Sedation
Tell every provider before any procedure requiring anesthesia or deep sedation that you take Zepbound. The FDA states that available data are insufficient to recommend a specific fasting change or a temporary hold. Your anesthesiologist makes that call, and they cannot make it if they do not know.
Pregnancy and Breastfeeding
Weight loss offers no benefit during pregnancy and may harm the fetus. Discontinue Zepbound when pregnancy is recognized. In a lactation study, tirzepatide was undetectable in most breast milk samples, but data on effects in a breastfed infant do not exist.
Existing Kidney, Pancreas, or Thyroid Conditions
Zepbound is not recommended in patients with severe gastroparesis. A history of pancreatitis, diabetic retinopathy, or any thyroid nodule changes the calculus and belongs in the conversation before dose one, not after symptom one.
Long-Term Safety and Monitoring While You’re on Zepbound
What the Long-Term Data Shows
Extended follow-up from the SURMOUNT-1 program out to 176 weeks reported serious adverse events in 12.6% to 14.5% of tirzepatide participants against 11.9% on placebo, with treatment discontinuation due to adverse events in 7.3% to 12.3% versus 5.9%. Pancreatitis occurred in 0.4% of both the tirzepatide and placebo groups.
No SURMOUNT trial has followed patients beyond 88 weeks in the main program, which means late-emerging effects remain genuinely unmeasured. That is a limitation, and anyone telling you the long-term safety question is closed is overselling.
Real Life Is Not the Trial
A Cleveland Clinic cohort of 7,881 adults found that 16.4% of tirzepatide users stopped within three months and another 34.1% stopped between three and twelve months. More than 80% never climbed past a low maintenance dose.
Their one-year weight loss averaged 12.4%, against the 20.9% seen in the trial. Side effects, cost, and expectations all feed that gap, and none of them are medical failures. They are human ones.
The financial pressure is real. Zepbound’s list price sits above $1,000 per month, with manufacturer self-pay routes running roughly $299 to $449. When a person is paying that out of pocket, the decision to push through a rough dose increase stops being purely clinical.
Baseline Labs Worth Having Before Dose One
Most people start this drug with no reference point, which is a missed opportunity, because several of its serious side effects show up in bloodwork before they show up in symptoms.
A thyroid profile, kidney function panel, liver function test, HbA1c, fasting glucose, and lipid profile give you that reference point. Zepbound raises serum amylase by 20% to 25% and lipase by 28% to 35% on average, and the label states the clinical meaning of those elevations is unknown without other signs of pancreatitis. Which is exactly why a baseline matters. Without one, a routine elevated lipase becomes a frightening unknown instead of an expected shift.
What To Recheck and When
Kidney function after any episode of prolonged vomiting or diarrhea. HbA1c and a lipid profile at three to six months to document the metabolic payoff, which is often larger than the scale suggests. Iron, ferritin, and vitamin B12 if hair shedding starts.
Our lab partners report that the patients who bring a baseline panel to their follow-up appointment have a materially easier conversation with their prescriber, because the question shifts from “is this the drug?” to “here is what changed.”
In cases reviewed across our diagnostic network, tracking these markers alongside the scale is what separates a patient who can tell a drug effect from a coincidence, and a patient who quits over a symptom that had nothing to do with Zepbound at all.
Frequently Asked Questions
How long do Zepbound side effects last?
Most gastrointestinal symptoms appear within days of starting or increasing your dose and settle over roughly one to two weeks. The FDA notes that most nausea, vomiting, and diarrhea occurred during dose escalation and decreased over time. Once you hold a stable maintenance dose, symptoms usually quiet down substantially.
When do Zepbound side effects start?
Typically within the first week of your first injection, and again within 24 to 72 hours of each dose increase. Pooled SURMOUNT trial data confirm gastrointestinal events were reported primarily during dose escalations. Because the ladder runs about 20 weeks, expect several separate waves rather than one long stretch.
What is the most common side effect of Zepbound?
Nausea. It affected 25% at 5 mg, 29% at 10 mg, and 28% at 15 mg, against 8% on placebo. Real-world numbers run higher: RAND found 52% of GLP-1 users reported nausea, though most rated it mild rather than serious.
Which Zepbound dose has the fewest side effects?
Not the one you would guess. Overall gastrointestinal reactions ran 56% at 5 mg, 10 mg, and 15 mg alike. Vomiting rises with dose while constipation falls. What lowers your risk is a slower climb, not a permanently lower ceiling.
Does Zepbound cause hair loss?
Yes, and the sex difference is striking. Hair loss was reported in 7.1% of women versus 0.5% of men on Zepbound, and the FDA associates it with weight reduction rather than a direct drug effect. No patient in the trials stopped treatment because of it, and it typically resolves.
Why does Zepbound cause sulfur burps?
Slowed gastric emptying leaves protein-rich food fermenting longer in the stomach, and gut bacteria produce hydrogen sulfide gas. The label reports burping in 4% to 5% of patients versus 1% on placebo. Cutting high-sulfur foods and carbonated drinks around injection day usually helps within days.
Does Zepbound cause muscle loss?
Some, but no more proportionally than ordinary dieting. In the SURMOUNT-1 DXA substudy, roughly 75% of the weight lost was fat and 25% was lean mass, the identical ratio seen in the placebo group. Protein intake and resistance training remain the standard defense.
Can Zepbound cause pancreatitis?
It carries a warning, but trial rates are low. Adjudicated acute pancreatitis occurred in 0.2% of Zepbound patients and 0.2% of placebo patients. Severe, persistent abdominal pain radiating to the back means stop the drug and seek emergency care immediately.
Is Zepbound safe long term?
Extended SURMOUNT-1 follow-up to 176 weeks showed serious adverse events in 12.6% to 14.5% of tirzepatide participants against 11.9% on placebo. No trial has run past 88 weeks in the core program, so effects emerging after several years remain unstudied rather than ruled out.
Can you drink alcohol on Zepbound?
There is no formal contraindication, but alcohol irritates the stomach, dehydrates, and lowers blood pressure. Since Zepbound already slows gastric emptying and was linked to hypotension in 1.6% of patients, alcohol tends to amplify nausea, reflux, and dizziness. Discuss it with your prescriber.
Does Zepbound affect birth control pills?
Yes. The FDA advises switching to a non-oral contraceptive method, or adding a barrier method, for four weeks after starting Zepbound and for four weeks after each dose increase. With a 20-week escalation schedule, that means several separate windows of reduced protection.
Do side effects mean Zepbound is working?
No, and this myth causes real harm. Weight loss was nearly the same in trial participants who experienced gastrointestinal side effects and in those who did not. Feeling sick is not evidence of effectiveness, and pushing through severe symptoms buys you nothing but risk.
Medical Disclaimer
This article is for educational purposes and does not replace advice from a licensed healthcare provider. Zepbound is a prescription medication carrying a boxed warning and several serious risks. Do not start, stop, or adjust your dose without consulting your prescriber. If you experience severe abdominal pain, persistent vomiting, or signs of an allergic reaction, seek emergency medical care immediately. Report side effects to FDA MedWatch at 1-800-FDA-1088.
References
- FDA Zepbound (tirzepatide) Prescribing Information, revised February 2026
- FDA Drug Safety Communication: Removal of Suicidal Behavior and Ideation Warning from GLP-1 Receptor Agonist Medications, January 2026
- FDA: Concerns with Unapproved GLP-1 Drugs Used for Weight Loss
- RAND Corporation: GLP-1 Agonist Use and Side Effects in the United States, 2025
- KFF Health Tracking Poll: GLP-1 Use, November 2025
- Body Composition Changes During Weight Reduction with Tirzepatide: SURMOUNT-1 DXA Substudy, Diabetes, Obesity and Metabolism
- Gastrointestinal Tolerability of Tirzepatide Across SURMOUNT-1 to -4, Diabetes, Obesity and Metabolism
- American College of Cardiology: SURMOUNT-5, Tirzepatide vs Semaglutide
- Real-World GLP-1 Weight-Loss Outcomes and Discontinuation, Cleveland Clinic Cohort (Obesity, 2025)
- Tirzepatide for Overweight and Obesity Management: Long-Term Safety Review
- CDC National Center for Health Statistics: GLP-1 Injectable Use Among US Adults with Diagnosed Diabetes
- Zepbound Official Side Effects Information, Eli Lilly and Company