
A blood test came back normal. The tingling in her hands did not.
That gap, between a lab result that says everything is fine and a body that clearly disagrees, is the most misunderstood thing about vitamin B12 deficiency. And it may be about to get a lot more attention.
Table of Contents
Researchers at UC San Francisco enrolled 231 healthy older adults, average age 71, every single one with a B12 level above the deficiency cutoff. The participants sitting toward the lower end of “normal” still showed impaired brain processing speed, delayed responses to visual stimuli, and more white matter damage on MRI.
They were all normal. They were also, measurably, not fine.
Quick Answer
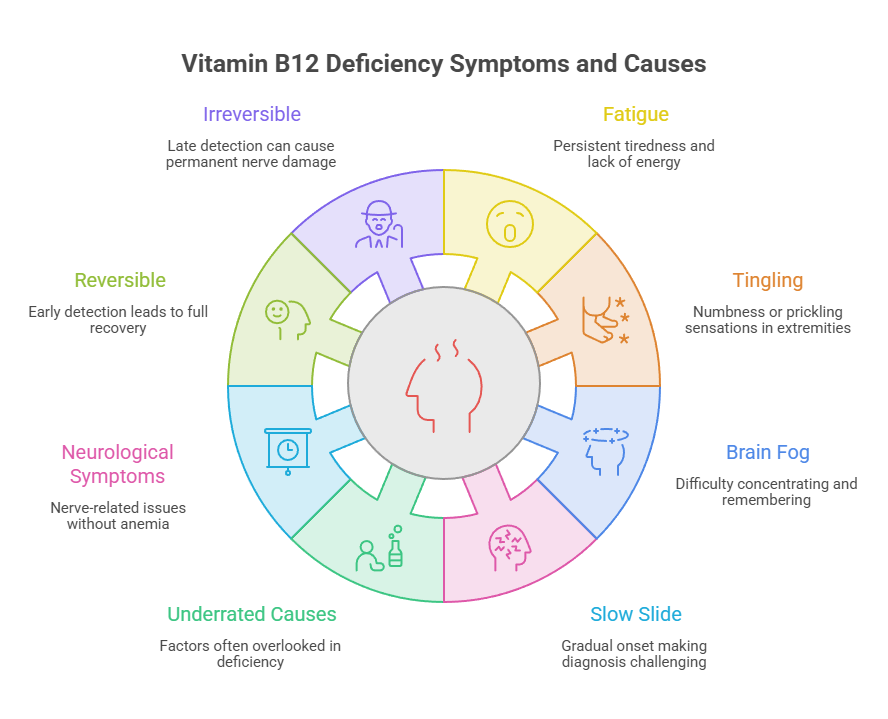
Vitamin B12 deficiency happens when your body does not get enough B12, or cannot absorb what it gets. The most common signs are fatigue, tingling or numbness in the hands and feet, brain fog, mouth soreness, and pale skin. Most labs call serum B12 under 200 to 250 pg/mL deficient, but symptoms often appear in the 200 to 300 pg/mL “normal” range, and neurological damage can start before anemia ever shows up.
At a Glance
- Roughly 3.6% of US adults are deficient (under 200 pg/mL), and 12.5% are insufficient (under 300 pg/mL).
- Fatigue, tingling, and brain fog lead the symptom list, and all three get blamed on stress or aging.
- Neurological symptoms can occur without anemia, so a normal blood count rules out nothing.
- Serum B12 alone is a weak test. Methylmalonic acid and active B12 catch what it misses.
- Metformin, acid reducers, and recreational nitrous oxide are the underrated causes.
- Your liver stores enough B12 to last years, which is why the slide is slow and easy to misread.
- Caught early, this is fully reversible. Caught late, some nerve damage is not.
What Vitamin B12 Actually Does (and Why Running Out Hurts So Much)
Vitamin B12, also called cobalamin, is the only vitamin that contains a metal atom. Cobalt sits at its center, and that detail matters more than it sounds.
B12 is required for the development, myelination, and function of the central nervous system, for healthy red blood cell formation, and for DNA synthesis. Three jobs. When supply drops, all three degrade at once.
Two Enzymes, and Why Nerves Pay First
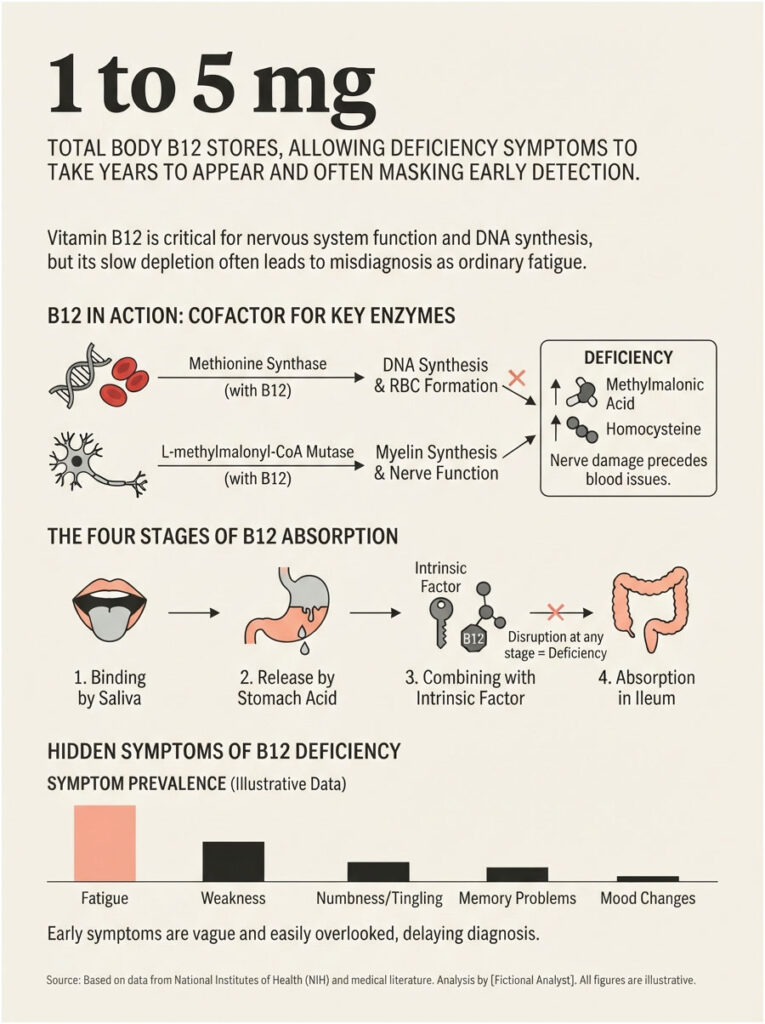
B12 acts as a cofactor for exactly two enzymes: methionine synthase and L-methylmalonyl-CoA mutase. That is the entire job description.
Without enough B12, methylmalonic acid backs up and homocysteine climbs. Myelin, the insulation wrapped around your nerve fibers, stops being maintained. The wiring frays before the blood does.
Our medical reviewers see this pattern constantly. A patient arrives convinced they have a circulation problem or early neuropathy, and the actual answer is a vitamin their body quietly stopped absorbing four years ago.
The Absorption Relay
Getting B12 out of food and into your bloodstream takes four separate handoffs. Saliva binds it. Stomach acid and gastric protease release it from the food matrix. It then combines with intrinsic factor, a protein secreted by the stomach’s parietal cells, and is finally absorbed in the distal ileum.
Break any link and the whole chain fails. Low stomach acid, no intrinsic factor, or a damaged small intestine all produce the same outcome.
Why You Can Coast for Years
Here is the reason this condition hides so well. The body stores about 1 to 5 milligrams of B12, roughly 1,000 to 2,000 times the amount you consume in a day, so symptoms can take several years to appear.
You do not fall off a cliff. You drift down a very long ramp, and every step feels like ordinary tiredness.
The Common Signs of Vitamin B12 Deficiency
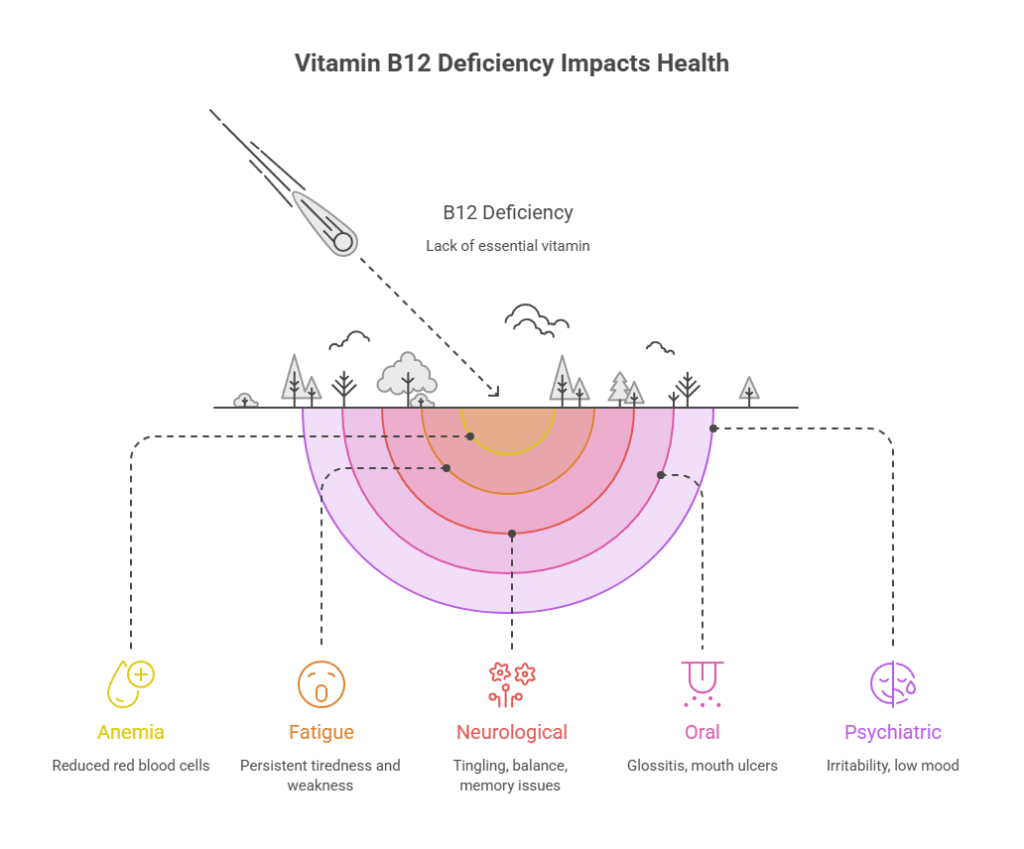
The classic picture includes megaloblastic anemia with large abnormal red blood cells, glossitis of the tongue, fatigue, palpitations, pale skin, weight loss, and neurological changes such as numbness and tingling in the hands and feet.
That is the textbook version. Real patients rarely arrive with the full set.
Consider a case Harvard Health highlighted from Massachusetts General Hospital, published in the New England Journal of Medicine. Over two months, a 62-year-old man developed numbness and a pins-and-needles sensation in his hands, had trouble walking, experienced severe joint pain, began turning yellow, and grew progressively short of breath. The cause was a lack of vitamin B12.
Not one of those symptoms says “vitamin” to a patient. Together, they nearly cost him his nervous system.
The Early Signs
Fatigue that sleep does not fix. Breathlessness on a single flight of stairs. Dizziness on standing. Skin that has gone pale, or in some cases faintly yellow.
With B12-deficiency anemia you may notice the typical anemia symptoms first, including fatigue, paleness, shortness of breath, headaches, and dizziness. These are the signs people explain away the longest.
The Neurological Signs
Pins and needles in the hands and feet. Numbness that creeps upward. Trouble with balance, especially in the dark. Memory lapses, word-finding problems, and a sense that your thinking has slowed.
Neuropsychiatric symptoms may precede the blood signs entirely, presenting as myelopathy, neuropathy, dementia, and less often optic nerve atrophy. Nerves do not wait for your blood count to give permission.
The Mouth and Tongue Signs
A sore, smooth, beefy-red tongue is called glossitis, and it is one of the more specific clues on the list. Mouth ulcers, a burning sensation, and cracks at the corners of the lips often travel with it.
The Mood and Psychiatric Signs
Irritability. Low mood. Anxiety with no obvious trigger. In severe cases B12 deficiency has produced depression, psychosis, delirium, and cognitive decline severe enough to be mistaken for dementia.
The Signs Almost Nobody Connects
Heart palpitations. Vision changes. Darkening of the skin, especially across the knuckles, which has occasionally been the only presenting sign of early B12 deficiency.
Patients booking B12 panels with us are routinely surprised by that last one. They came in for fatigue and never thought to mention their hands.
Table A: Signs of B12 Deficiency by Body System and Stage
| Sign | Body System | What’s Going Wrong | When It Appears |
| Persistent fatigue, weakness | Blood | Fewer functional red blood cells carrying oxygen | Early to mid |
| Shortness of breath on exertion | Blood | Reduced oxygen delivery to working muscle | Mid |
| Pale or yellow-tinged skin | Blood | Anemia plus red cell breakdown raising bilirubin | Mid to late |
| Heart palpitations | Cardiovascular | Heart compensating for low oxygen-carrying capacity | Mid to late |
| Tingling, pins and needles in hands or feet | Peripheral nerves | Myelin sheath degrading around nerve fibers | Early to mid |
| Numbness, loss of sensation | Peripheral nerves | Progressive demyelination and axonal damage | Mid to late |
| Poor balance, unsteady walking | Spinal cord | Subacute combined degeneration of the posterior columns | Late |
| Brain fog, slow thinking, memory lapses | Brain | Impaired myelination and rising homocysteine | Early to late |
| Depression, irritability, anxiety | Brain | Disrupted methylation and neurotransmitter synthesis | Early to mid |
| Sore, smooth, red tongue (glossitis) | Mouth | Rapidly dividing cells fail without B12 for DNA synthesis | Early to mid |
| Mouth ulcers, burning mouth | Mouth | The same DNA synthesis failure in oral mucosa | Early to mid |
| Darkened skin over the knuckles | Skin | Altered melanin distribution | Variable, uncommon |
The Most Dangerous Myth: “My Blood Count Was Fine, So It Isn’t B12”
This is the single belief that costs people their nerves.
Neurological symptoms can occur without anemia, which is exactly why early diagnosis matters for avoiding irreversible damage. In one study of 141 consecutive patients with neuropsychiatric symptoms from B12 deficiency, 28% had a normal hematocrit, a normal mean corpuscular volume, or both.
More than a quarter of them looked hematologically healthy while their nervous system was under attack.
What Your B12 Number Actually Means
Most laboratories define subnormal serum B12 as under 200 or 250 pg/mL, though the cutoff varies by method and by lab. That one sentence hides an enormous amount of clinical trouble.
Table 1: Serum B12 Zones, Decoded
| Serum B12 (pg/mL) | Serum B12 (pmol/L) | Lab Verdict | What It Actually Means | Recommended Next Step |
| Under 150 | Under 111 | Deficient | Clear deficiency. Neurological damage is possible right now. | Treat immediately and find the cause. |
| 150 to 199 | 111 to 147 | Deficient (most labs) | Deficiency. Anemia may or may not be present. | Treat. Order MMA, homocysteine, CBC, folate. |
| 200 to 299 | 148 to 220 | “Normal” | The gray zone. Symptoms are common here. | Order MMA. Do not stop at the B12 number. |
| 300 to 399 | 221 to 294 | Normal | Usually adequate, but functional deficiency is still possible. | NIH advises checking MMA anywhere from 150 to 399 pg/mL if suspicion remains. |
| 400 to 600 | 295 to 442 | Normal | Generally reassuring when there are no symptoms. | Retest only if symptoms persist. |
| 600 to 813 | 443 to 600 | Normal to high | Common with supplementation. Says nothing about cellular status. | If symptomatic, measure MMA and active B12. |
| Above 813 | Above 600 | High | Can reflect liver disease, alcohol use, or supplements. In an analysis of 757,185 people, adjusted 1-year cancer risk ran 1.74 to 4.72 times higher above this level. | Investigate the cause. High is not “extra healthy.” |
Source: NIH Office of Dietary Supplements, Vitamin B12 Fact Sheet for Health Professionals
Why the Number Moves Depending on Who Is Counting
Change the cutoff and you change the epidemic. Among US adults in NHANES, the rate of low serum B12 was 3% at a cutoff of 200 pg/mL and 26% at a cutoff of 350 pg/mL.
Same population. Same blood. Eight times the diagnosis rate, purely from where somebody drew a line.
The Gray Zone, and the Test That Resolves It
Experts advise that when serum B12 lands between 150 and 399 pg/mL, methylmalonic acid should be measured to help confirm the diagnosis.
In tests booked through HealthCareOnTime, this is the step most often skipped. A patient comes back at 240, gets told they are fine, and walks out with nothing resolved and every symptom intact.
Why a “Normal” B12 Result Can Still Be Wrong
Serum B12 measures how much vitamin is circulating in your blood. It does not measure how much is reaching your cells.
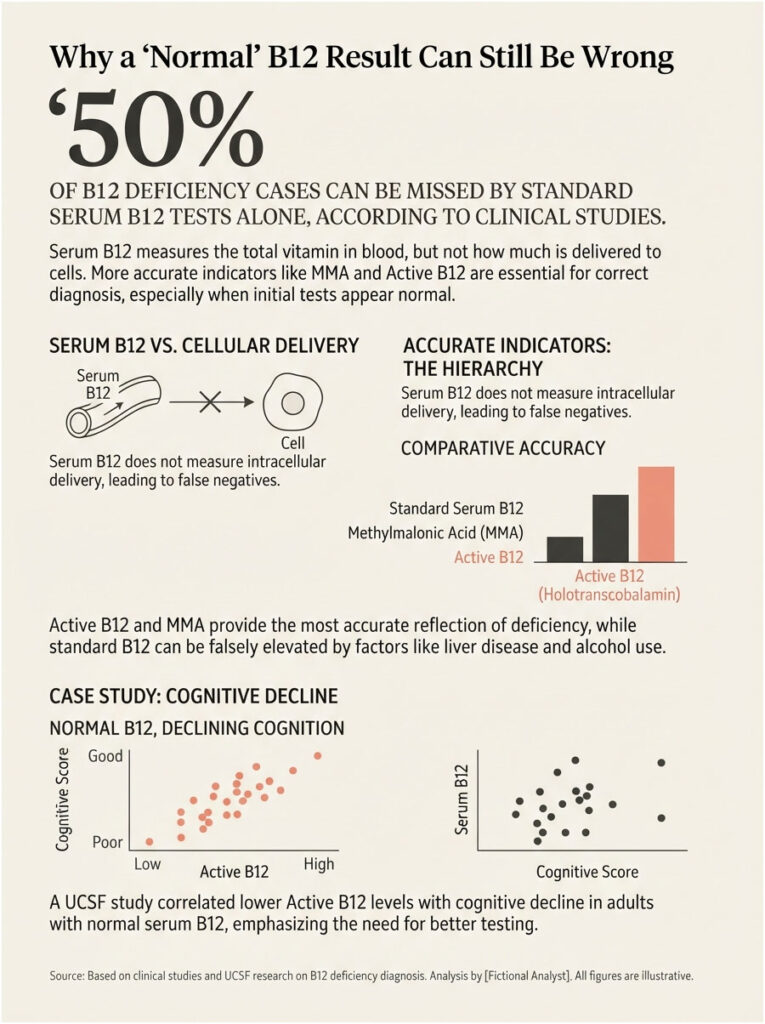
Numerous studies have established that serum B12 has limited diagnostic value as a stand-alone marker, and severe functional deficiency has been documented in people with normal and even high serum B12.
The Four Markers That Tell the Real Story
Serum B12 is the screening test. Cheap, universal, and blunt.
Methylmalonic acid (MMA) is the most sensitive marker of B12 status. A level above 0.271 micromol/L suggests deficiency. It rises when your cells run short, even while your blood looks fine.
Homocysteine rises quickly as B12 status declines, with levels above 15 micromol/L suggesting deficiency. Specificity is poor, because folate status and kidney function both move it.
Active B12, also called holotranscobalamin, is the fraction actually delivered to your cells. In a study of 11,833 samples, holotranscobalamin had the highest diagnostic accuracy for subclinical deficiency, and in women aged 50 and older it outperformed serum B12, MMA, and homocysteine.
What Falsely Raises Your B12
Liver disease. Heavy alcohol use. A B12 supplement taken the week before the draw. All three can push a serum result into the comfortable range while your cells are starving.
When MMA Lies Too
Honesty about the limits matters. MMA levels also rise with kidney impairment and tend to run higher in older adults.
In renal failure, MMA can climb to 300 to 700 nmol/L and stay elevated even after B12 treatment. Which means an MMA result should always be read next to your kidney function, not in isolation.
There is no perfect single test here. There is only a panel, read together, by someone paying attention.
The Study That Put “Normal” on Trial
The UCSF work deserves a closer look. Researchers recruited 231 healthy adults with no dementia or mild cognitive impairment through the Brain Aging Network for Cognitive Health, average age 71, median B12 concentration around 414.8 pmol/L, comfortably inside the normal range.
Lower active B12 in that group tracked with slower thinking, slower visual processing, and more visible injury to the brain’s white matter. The investigators concluded that redefining B12 deficiency around functional biomarkers could allow earlier intervention and the prevention of cognitive decline.
Read that again. The threshold itself may be set too low.
The Folic Acid Problem, and Why It Is Uniquely American
Since January 1998, the FDA has required folic acid fortification of all enriched cereal-grain products, mainly to prevent neural tube birth defects. As public health programs go, it worked.
It also disabled an early warning system. In the 1940s and 1950s, high-dose folic acid was used to reverse the megaloblastic anemia of B12 deficiency, but that treatment masked the underlying deficiency and possibly worsened its neurological progression.
Folic acid can partially rescue the effects of B12 deficiency on anemia, but it is not known to rescue the effects on neurological pathology. The anemia gets patched. The nerves keep degrading.
People with low B12 and elevated folate score lower on cognitive tests and show higher homocysteine and MMA than people with low B12 and normal folate. NHANES data on 2,420 US adults aged 60 and older found that low B12 combined with high folic acid was associated with roughly two to three times higher risk of cognitive impairment.
In America, the red flag that used to appear on a routine blood count often never appears at all.
Who Actually Gets B12 Deficiency in the US
Table 2: US Prevalence and Risk by Group
| Group | Deficiency or Risk Rate | Why This Group | Source |
| All adults 19+ | 3.6% deficient (under 200 pg/mL); 12.5% insufficient (under 300 pg/mL) | Baseline population risk | NHANES 2007-2018, Am J Clin Nutr |
| Adults 60+ | 3.7% deficient; 12.3% insufficient; about 21% abnormal on at least one biomarker | Declining stomach acid and intrinsic factor | NIH ODS, updated July 2025 |
| Community-dwelling older adults | 3% to 43%, depending on the cutoff used | Atrophic gastritis and medication load | NIH ODS |
| Long-term metformin users | 19.1% low or borderline-low at 5 years, vs 9.5% on placebo | Metformin impairs B12 absorption | DPPOS, J Clin Endocrinol Metab |
| Metformin, past 10 years of use | 8.1% deficient, vs 4.1% at 3 to 10 years | Risk compounds with duration | NHANES analysis |
| People with pernicious anemia | 15% to 25% of B12 deficiency in older adults; US incidence about 151 per 100,000 | Autoimmune loss of intrinsic factor | NIH ODS |
| Adults 65+ with atrophic gastritis | 8% to 9% of that age group, vs 2% of the general population | Reduced acid and intrinsic factor output | NIH ODS |
| Recreational nitrous oxide users | About 4.6% of Americans aged 12+ have misused nitrous oxide | Nitrous oxide inactivates B12 directly | FDA safety alert 2025; Cureus |
Older Adults and the Atrophic Gastritis Problem
The stomach quietly stops cooperating. Atrophic gastritis affects about 2% of the general population but 8% to 9% of adults aged 65 and older, cutting both intrinsic factor production and hydrochloric acid secretion.
Diet has nothing to do with it. You can eat steak every night and still absorb almost none of it.
Pernicious Anemia: The Autoimmune Cause Hiding in Plain Sight
Pernicious anemia is an irreversible autoimmune disease in which the body attacks the parietal cells of the stomach, destroying intrinsic factor production. It is the most common cause of clinically evident B12 deficiency worldwide, and it is more common in women and in people of European ancestry.
The insidious part is the timeline. Asymptomatic autoimmune gastritis precedes the onset of stomach lining atrophy by 10 to 20 years.
Two decades of silence, then symptoms. It also carries an elevated long-term risk of gastric cancer, driven by the same chronic inflammation and low stomach acid, which is why the diagnosis is worth pinning down rather than papering over with supplements.
The Iron Deficiency That Comes First
Here is a clue almost nobody catches. As parietal cells die off, stomach acid falls first, and stomach acid is required to absorb iron. So pernicious anemia may present initially as iron deficiency anemia, years before the B12 problem shows up.
Across the patients we serve, an unexplained iron deficiency in an older adult with no bleeding source is one of the most reliable prompts to look at B12 and intrinsic factor antibodies.
Why Women Are Hit Differently
Women eat less B12 to begin with. Mean daily intake from food runs 5.84 mcg for men aged 20 and older versus 3.69 mcg for women, and 11% of US women fall below the estimated average requirement compared with 5% of men.
Pernicious anemia is more common in women. B12 needs rise during pregnancy and breastfeeding. And after age 50, active B12 outperforms every other marker as a first-line test in women.
Which means the standard workup, a single serum B12 with no follow-up, is least reliable in exactly the group most likely to be affected.
The Causes Nobody Talks About
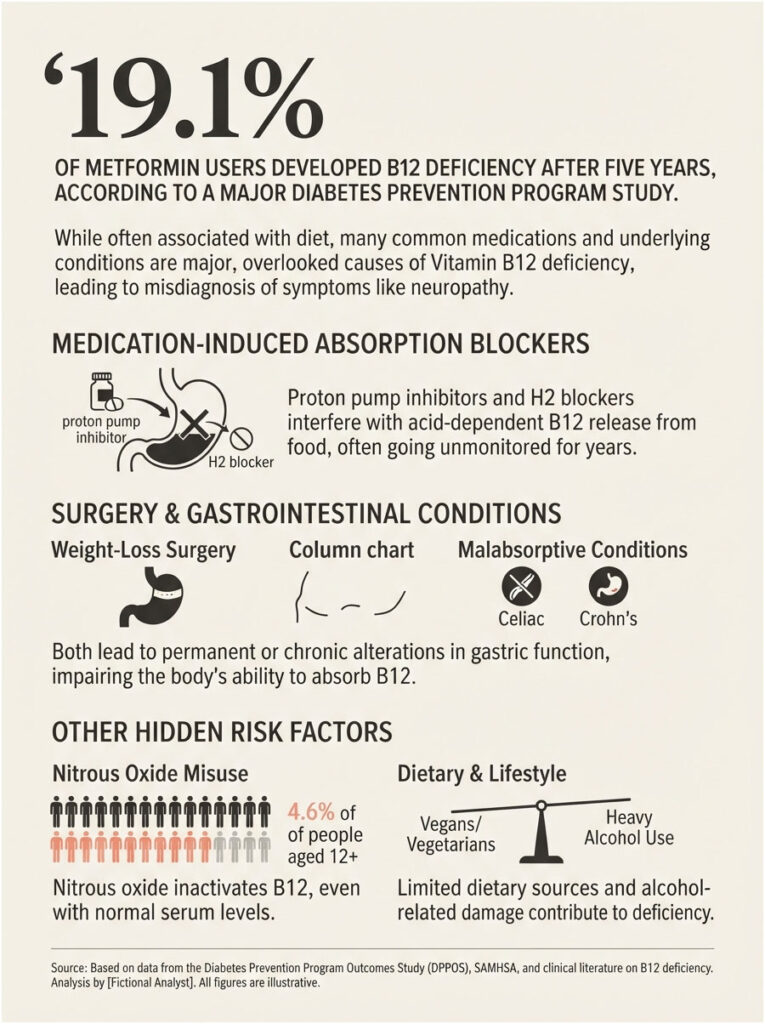
Metformin
Metformin is the first-line drug for prediabetes and type 2 diabetes, which makes it one of the most-prescribed medications in the country. Almost no one taking it is told about this.
In the Diabetes Prevention Program Outcomes Study, low B12 occurred more often in the metformin group than placebo at 5 years (4.3% vs 2.3%), and combined low plus borderline-low B12 was far more common in metformin users at both 5 years (19.1% vs 9.5%) and 13 years (20.3% vs 15.6%). Mean B12 ran 10% lower in the metformin group.
Each additional year of metformin use raised the odds of B12 deficiency by 13%, and neuropathy was more prevalent among metformin users with low B12.
Read that last clause twice. A person on metformin with numb feet may be told it is diabetic neuropathy when it is actually a treatable vitamin deficiency the drug caused. The American Diabetes Association recommends considering periodic B12 assessment in patients on long-term metformin, including those with prediabetes, peripheral neuropathy, or anemia.
Acid Reducers
Proton pump inhibitors such as omeprazole (Prilosec) and lansoprazole (Prevacid), and H2 blockers such as cimetidine (Tagamet), interfere with B12 absorption from food by slowing gastric acid release, and can lead to deficiency over time.
These are among the most-prescribed drugs in America, and plenty of people take them for a decade without a single B12 check.
Nitrous Oxide, the Fastest-Moving Cause in America
On March 14, 2025, the FDA warned consumers not to inhale or recreationally use nitrous oxide in any canister, tank, or charger, listing vitamin B12 deficiency alongside numbness, tingling, limb weakness, paralysis, trouble walking, and psychiatric disturbances among the resulting harms. The agency also noted that regular inhalation can cause prolonged neurological effects, including spinal cord or brain damage, even after use stops.
In the United States, 4.6% of people aged 12 and older have misused nitrous oxide. The gas inactivates vitamin B12 by oxidizing its cobalt ion.
Why the Blood Test Lies in These Cases
This is the part that catches clinicians off guard. Nitrous oxide does not lower your B12. It breaks the B12 you already have.
The vitamin is still in your bloodstream, still measurable, still normal on a serum test. It just no longer works. One reported case involved a 22-year-old with a B12 level of 180 pg/mL, progressive stiffness and tingling, and MRI showing abnormal signal in the brain and the posterior spinal cord.
Anyone using nitrous oxide recreationally who develops numbness or balance problems needs MMA and homocysteine measured, not just serum B12.
Weight-Loss Surgery
Gastrointestinal procedures such as bariatric surgery, or removal of part of the stomach, cause partial or complete loss of the cells that secrete hydrochloric acid and intrinsic factor, reducing B12 absorption.
The plumbing changes permanently. So does the supplementation requirement.
The Rest of the List
Celiac disease and Crohn’s disease can impair absorption. H. pylori infection is associated with deficiency in older adults, likely through inflammation-driven malabsorption. Vegans and vegetarians carry elevated risk because natural food sources are limited to animal products. Heavy alcohol use interferes as well.
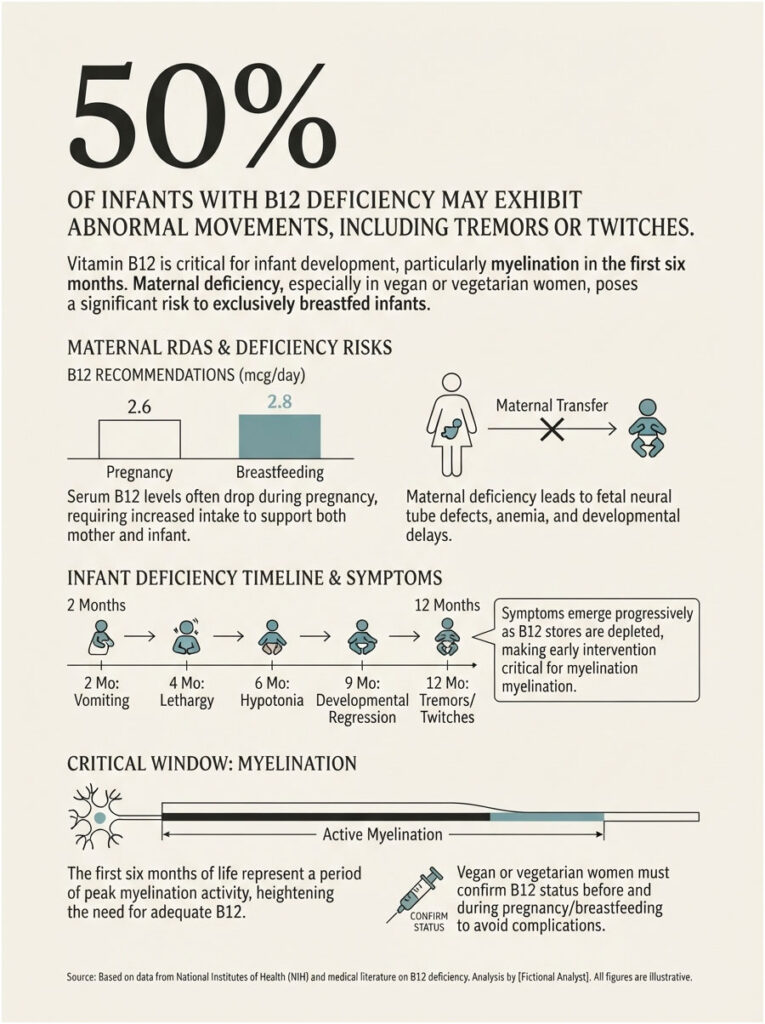
Pregnancy, Breastfeeding, and Infants
This is the section most articles skip, and it is the one with the highest stakes.
What Happens During Pregnancy
Serum B12 tends to drop during pregnancy, sometimes into subnormal territory, and usually returns to normal after delivery. The RDA rises to 2.6 mcg in pregnancy and 2.8 mcg while breastfeeding.
That dip complicates interpretation. A borderline result in a pregnant patient needs the full panel, not a shrug.
The Risk to the Baby
In pregnant and breastfeeding women, vitamin B12 deficiency may contribute to neural tube defects, developmental delays, failure to thrive, and anemia in the child.
Exclusively breastfed infants of women who eat no animal products can have very limited B12 reserves and may become deficient early in life. Undetected and untreated infant deficiency can cause neurological damage, failure to thrive, developmental delays, and anemia.
The mother’s own deficiency is sometimes clinically mild and completely unrecognized.
Warning Signs in an Infant
Symptoms typically appear between 2 and 12 months and include vomiting, lethargy, failure to thrive, low muscle tone, and the arrest or regression of developmental skills. Roughly half of affected infants show abnormal movements such as tremors, twitches, or myoclonus.
Myelination is most active in the first six months of life, which is why infantile B12 deficiency can do so much damage so fast. Treatment corrects the metabolic abnormalities within days.
Our medical team’s position is straightforward: any vegan or vegetarian who is pregnant or breastfeeding should have B12 status confirmed, not assumed.
The Four Stages: How Deficiency Sneaks Up on You
Deficiency is not a switch. It is a staircase, and you can be several steps down before anything hurts.
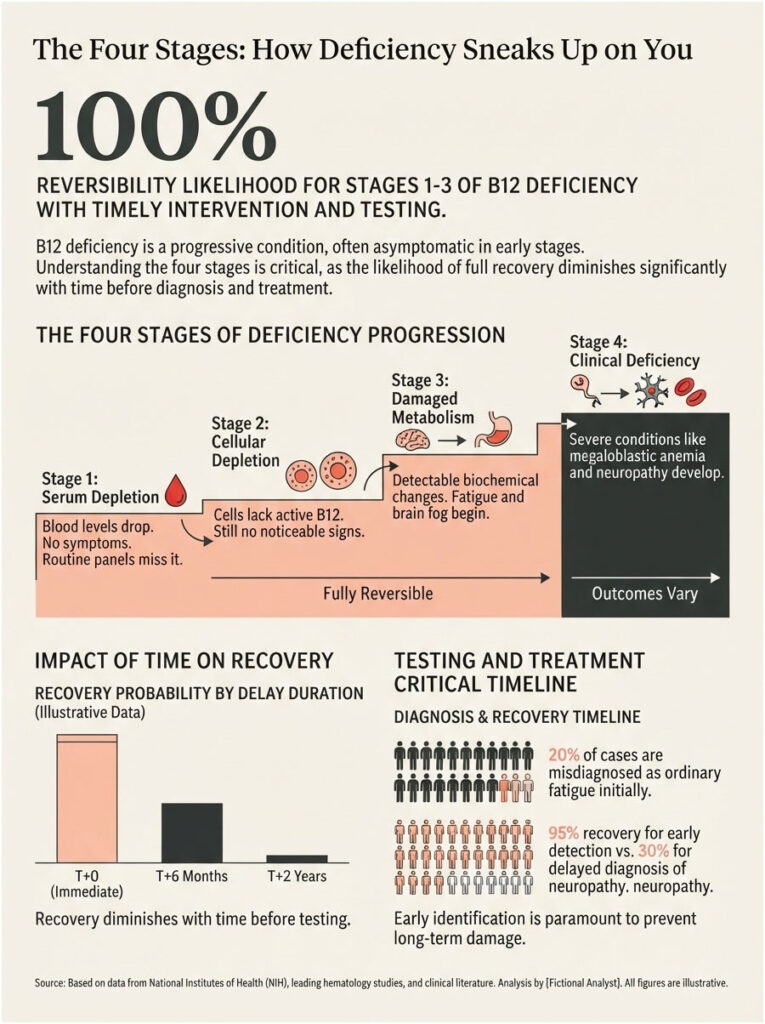
Stage 1: Serum Depletion
Blood levels begin to fall, with active B12 dropping first. No symptoms. Nothing on a routine panel would catch it.
Stage 2: Cellular Depletion
Cells start running short and cellular function begins to slip. Still no clear signs. Active B12 is now low while serum B12 may still read normal.
Stage 3: Damaged Metabolism
Biochemical changes become detectable. MMA climbs. Homocysteine climbs. Fatigue, brain fog, and the first tingling usually begin here, and this is where most people are still being told they are fine.
Stage 4: Clinical Deficiency
Megaloblastic anemia. Frank neuropathy. In the spinal cord this appears as subacute combined degeneration, with symmetric abnormal sensation, loss of position sense, and spastic weakness.
Where the Reversibility Line Sits
Everything through Stage 3 typically reverses fully with treatment. Stage 4 is a coin toss, and some brain and nerve symptoms such as numbness and tingling may never fully go away, even with treatment.
In cases reviewed by our medical team, the difference between full recovery and permanent deficit is almost never the severity of the deficiency. It is how many months passed before anyone tested for it.
Should You Get Tested, and Which Test Should You Ask For?
Table 3: Scenario, Risk, Test to Request, Next Step
| Your Situation | Risk Level | Test to Request | Recommended Action |
| On metformin 3+ years | High | Serum B12 + MMA | Test annually. Discuss supplementation regardless of the result. |
| On a PPI or H2 blocker 1+ year | Moderate to High | Serum B12 + MMA | Test now, then annually. Ask whether you still need the drug. |
| Vegan or vegetarian 2+ years, not supplementing | High | Serum B12 + MMA | Test now. Start a reliable B12 source immediately. |
| Over 60 with fatigue or memory changes | High | Serum B12 + MMA + CBC + folate | Test before accepting that it is just aging. |
| Pregnant or breastfeeding on a plant-based diet | High | Serum B12 + MMA | Confirm status. Do not assume adequacy. |
| Post-bariatric surgery | Very High | Serum B12 + MMA, lifelong | Lifelong supplementation is the standard of care. |
| Tingling or numbness with a normal CBC | High | MMA + homocysteine + active B12 | A normal blood count does not clear you. Push for the metabolites. |
| Serum B12 came back 200 to 300 | Unresolved | MMA (mandatory) | This is the exact range where NIH advises confirming with MMA. |
| Serum B12 normal but symptoms persist | Unresolved | MMA + active B12 + kidney function | Functional deficiency exists at normal serum levels. Keep going. |
| Nitrous oxide use with neurological symptoms | Urgent | MMA + homocysteine + neuro exam | Serum B12 will mislead you here. Seek care promptly. |
What to Say to Your Doctor
Precision changes the outcome. Say it like this: your serum B12 sits in the gray zone, you have neurological symptoms, and you would like methylmalonic acid and homocysteine added to the order.
Our lab partners report that patients who arrive with a specific test request get a materially different workup than those who arrive with a vague complaint of tiredness. Naming the test is the whole trick.
What a Full Workup Includes
Serum B12. MMA. Homocysteine. A complete blood count with MCV. Serum folate. Kidney function, so the MMA can be read correctly.
If deficiency is confirmed, an intrinsic factor antibody test checks for pernicious anemia. Around 90% of pernicious anemia patients carry gastric parietal cell antibodies, but that test’s specificity is poor, since roughly 15% of older adults have them without the disease. The intrinsic factor antibody is the more decisive one.
How B12 Deficiency Is Treated (and How Fast It Works)
Injections vs Pills: What the Evidence Actually Says
B12 deficiency is typically treated with injections because that route bypasses every absorption barrier at once. Cyanocobalamin and hydroxocobalamin are both given this way, usually intramuscularly.
But a 2018 Cochrane Review of three randomized trials in 153 participants found that very high oral doses of 1,000 to 2,000 mcg normalized serum B12 about as well as intramuscular injections. Even after gastric bypass, 1,000 mcg per day of oral methylcobalamin appears as effective as hydroxocobalamin injections at restoring normal levels.
A prescription nasal gel also exists, with bioavailability around 2% at a 1,000 mcg dose, similar to oral.
The Absorption Math That Makes Pills Work Anyway
This is the part that makes everything click. Absorption runs about 50% at doses under 1 to 2 mcg, but only about 2% at a 500 mcg dose and 1.3% at 1,000 mcg.
Intrinsic factor saturates almost immediately. Past that point, a small fraction crosses the intestinal wall by passive diffusion, and passive diffusion does not care whether you have intrinsic factor at all.
Take 1,000 mcg and roughly 13 mcg still gets through. That is more than five times the daily requirement, which is precisely why oral B12 can rescue people who technically cannot absorb B12.
The Recovery Timeline
Blood counts usually begin correcting within weeks. Fatigue often lifts inside the first month. Nerve symptoms take months, improve the slowest, and may not fully reverse if the deficiency was prolonged.
Time is the only variable you actually control here.
When Treatment Is Lifelong
If the cause is pernicious anemia, bariatric surgery, or a medication you cannot stop, this is not a course of treatment. It is a permanent adjustment, and stopping resets the clock.
Food, Supplements, and What Actually Works
The RDA is 2.4 mcg for adults, 2.6 mcg in pregnancy, and 2.8 mcg while breastfeeding. That is a tiny amount, and most Americans clear it without trying. Only 5% of US men and 11% of women take in less than the estimated average requirement from food and beverages.
Which tells you something that reframes the entire condition: in the United States, deficiency is usually an absorption problem, not an eating problem.
Table 4: Best US Food Sources of Vitamin B12
| Food | B12 per Serving | Percent Daily Value |
| Beef liver, pan fried, 3 oz | 70.7 mcg | 2,944% |
| Clams, cooked, 3 oz | 17 mcg | 708% |
| Oysters, cooked, 3 oz | 14.9 mcg | 621% |
| Nutritional yeast, fortified, about 1/4 cup | 8.3 to 24 mcg | 346% to 1,000% |
| Salmon, Atlantic, cooked, 3 oz | 2.6 mcg | 108% |
| Tuna, light, canned in water, 3 oz | 2.5 mcg | 104% |
| Ground beef, 85% lean, 3 oz | 2.4 mcg | 100% |
| Milk, 2%, 1 cup | 1.3 mcg | 54% |
| Yogurt, plain, fat free, 6 oz | 1.0 mcg | 43% |
| Fortified breakfast cereal, 1 serving | 0.6 mcg | 25% |
| Egg, whole, 1 large | 0.5 mcg | 19% |
| Tempeh, 1/2 cup | 0.1 mcg | 3% |
| Spinach, beans, bananas, whole wheat bread | 0.0 mcg | 0% |
Source: NIH Office of Dietary Supplements, via USDA FoodData Central
Look at the bottom row. Plant foods contain no vitamin B12 unless they are fortified. No amount of spinach fixes this.
One more detail worth knowing: B12 bioavailability appears to be about three times higher from dairy than from meat, fish, or poultry, and about 50% higher from supplements than from food.
For Plant-Based Eaters
Fortified breakfast cereals and fortified nutritional yeasts are readily available, highly bioavailable sources, and using them alongside a supplement substantially reduces deficiency risk.
Fortification varies by brand, so read the label rather than trusting the category.
Which Form, and How Much
Cyanocobalamin is the most common form in supplements. No evidence indicates that absorption differs meaningfully by form, and sublingual tablets show no efficacy advantage over swallowed ones.
Multivitamins typically carry 5 to 25 mcg. B-complex products run 50 to 500 mcg. Standalone B12 supplements usually deliver 500 to 1,000 mcg, which is the range used to correct deficiency.
Can You Take Too Much?
No tolerable upper intake level has been set, because B12 has low potential for toxicity and the body does not hold onto the excess.
That said, a persistently high B12 reading is not a badge of health. It is a finding that deserves an explanation.
What Vitamin B12 Will Not Do for You
Honesty is part of the job, and there is a large industry selling B12 as an energy product on evidence that does not exist.
It Will Not Give You Energy If You Are Not Deficient
Because of its role in energy metabolism, B12 gets marketed as an energy enhancer and endurance booster. Supplementation appears to have no beneficial effect on performance in the absence of an actual nutritional deficit.
If your levels are normal, the shot is doing nothing but lightening your wallet.
It Will Not Prevent Heart Disease
A Cochrane Review covering 15 studies and 71,422 participants concluded that B12 supplements, alone or with other B vitamins, do not prevent heart attacks or reduce death rates in people at risk of or living with cardiovascular disease.
They lower homocysteine. They do not lower events.
It Will Not Improve Memory in People With Normal Levels
A Cochrane Review of 14 studies in 27,882 mostly older participants found that folic acid, B12, and B6 supplements had little to no effect on global cognitive function over five years, and no apparent impact over 5 to 10 years.
The entire value of B12 lies in correcting a deficiency you actually have. Which is exactly why testing matters more than supplementing blindly, and why a B12 shot bought without a blood test is a purchase, not a treatment.
Frequently Asked Questions
What is the most common sign of vitamin B12 deficiency?
Fatigue, followed closely by tingling or numbness in the hands and feet. The NIH lists fatigue, neurological changes, megaloblastic anemia, glossitis, palpitations, and low blood cell counts among the main effects. Fatigue is also the least specific symptom in medicine, which is exactly why deficiency goes unrecognized for years.
Can you have B12 deficiency with a normal blood test?
Yes, and this is the single most important thing to understand. Severe functional deficiency has been documented in people with normal and even high serum B12. If you have symptoms and a normal serum result, ask for methylmalonic acid and active B12 before accepting the answer.
What is a dangerously low B12 level?
Most labs treat anything under 200 pg/mL as deficient, and below 150 pg/mL treatment should not wait. But symptoms and nerve damage regularly occur in the 200 to 300 pg/mL range that labs still print as normal, which is why the number alone should never close the case.
How long does it take to become B12 deficient?
Usually years. The body stores 1 to 5 mg of B12, roughly 1,000 to 2,000 times a single day’s intake, so symptoms take several years to surface. The exception is nitrous oxide, which inactivates existing B12 directly and can produce severe neurological symptoms within weeks.
Can B12 deficiency cause permanent nerve damage?
Yes. Some brain and nerve symptoms, such as numbness and tingling, may not resolve even with treatment. Reversibility depends almost entirely on how long the deficiency went untreated. Caught within the first year, most people recover fully. Caught after years, some do not.
How long does it take to fix a B12 deficiency?
Blood counts typically begin normalizing within weeks and energy often improves within the first month. Nerve symptoms improve slowly over months and recover last, if they recover completely. The cause matters too: pernicious anemia requires lifelong treatment, not a temporary course.
Do B12 shots work better than pills?
Not necessarily. A Cochrane Review of three randomized trials found that high oral doses of 1,000 to 2,000 mcg normalized serum B12 about as well as intramuscular injections. Injections remain the default for severe deficiency or when adherence is uncertain, but high-dose oral works for most people.
Does metformin cause B12 deficiency?
It substantially raises the risk. In the DPPOS trial, low or borderline-low B12 affected 19.1% of metformin users versus 9.5% on placebo at 5 years, and every additional year of use raised deficiency odds by 13%. Anyone on long-term metformin should have B12 checked periodically.
Can vegans get enough B12 without supplements?
It is difficult and genuinely risky. Plant foods contain no B12 unless fortified, and vegans face higher deficiency risk because natural sources are limited to animal foods. Fortified cereals and nutritional yeast help, but a supplement is the reliable route. Test yearly rather than assuming.
Does B12 deficiency cause weight gain?
There is no strong evidence that it causes weight gain directly. Weight loss is actually among the recognized effects of deficiency. Fatigue can reduce activity levels, which may affect weight indirectly, but B12 is not a weight lever on its own in either direction.
Does vitamin B12 give you energy?
Only if you are deficient. Supplementation appears to have no beneficial effect on performance in the absence of a nutritional deficit. If your levels are normal, neither the shot nor the pill will make you feel more energetic. A blood test is the only way to know which situation you are in.
Can you take too much vitamin B12?
No tolerable upper intake level has been set, because B12 has low toxicity potential and the body does not store the excess. That said, a persistently elevated result is worth investigating rather than celebrating, since liver disease, alcohol use, and other conditions can drive it upward.
Medical Disclaimer
This article is for educational purposes and does not replace advice from a licensed healthcare provider. Do not start, stop, or change any medication or supplement based on what you read here. If you have numbness, tingling, balance problems, or memory changes, see a clinician promptly, because neurological damage from vitamin B12 deficiency can become permanent when treatment is delayed.
References
- NIH Office of Dietary Supplements: Vitamin B12 Fact Sheet for Health Professionals
- National Heart, Lung, and Blood Institute: Vitamin B12-Deficiency Anemia
- FDA: Advises Consumers Not to Inhale Nitrous Oxide Products, March 2025
- Long-term Metformin Use and Vitamin B12 Deficiency in the Diabetes Prevention Program Outcomes Study, Journal of Clinical Endocrinology and Metabolism
- UCSF: B12 Levels Within the Normal Range Linked to Cognitive Decline, Annals of Neurology
- Excess Folic Acid and Vitamin B12 Deficiency: Clinical Implications?
- Biomarkers and Algorithms for the Diagnosis of Vitamin B12 Deficiency, Frontiers in Molecular Biosciences
- Cobalamin Deficiency: Clinical Picture and Radiological Findings
- Nitrous Oxide-Induced Vitamin B12 Deficiency and Myelopathy in Whippets Abusers, Cureus
- Labcorp: Vitamin B12 Deficiency Cascade
- Cleveland Clinic: Vitamin B12 Deficiency
- Harvard Health: Vitamin B12 Deficiency Can Be Sneaky and Harmful





