

Nearly 9.5 million Americans land in an emergency room each year because their belly hurts, and abdominal pain now ranks as the single most common reason adults visit the ED in the United States. A surprising share of those visits trace back to one specific spot: the lower left side. That small patch of real estate hides your sigmoid colon, your left ureter, your left ovary or part of the left spermatic cord, and a stretch of small intestine. When something there goes wrong, you feel it fast.
Table of Contents
Quick Answer: Lower left abdominal pain most often comes from your sigmoid colon (diverticulitis, constipation, gas, IBS), your urinary tract (kidney stones, UTI), or in women, reproductive organs (ovarian cysts, endometriosis, ectopic pregnancy). Mild pain that fades in a day is usually harmless. Call 911 or head to an ER if pain is sudden and severe, comes with fever above 101°F, bloody stools, persistent vomiting, fainting, or a rigid, board-like belly.
At a Glance
- The sigmoid colon is the most common pain source in the lower left for adults over 40
- More than 30% of US adults aged 50 to 59 have diverticulosis; roughly 1 in 20 develop diverticulitis
- Kidney stones now affect about 11% of Americans, with rates climbing fastest among women
- About 6% of US adults meet Rome IV criteria for IBS, a condition that can mimic diverticular pain
- Pain lasting beyond 48 hours, worsening, or paired with fever or bleeding needs same-day medical evaluation
- Sex matters: women face ovarian and pregnancy-related causes men do not, and the reverse holds true
What Counts as “Lower Left Abdominal Pain”?
Picture a tic-tac-toe grid laid over your belly. The lower left square, what clinicians call the left lower quadrant (LLQ) or left iliac fossa, sits below your navel and to the left of your midline. It stretches from your left hip bone up to about belly-button level.
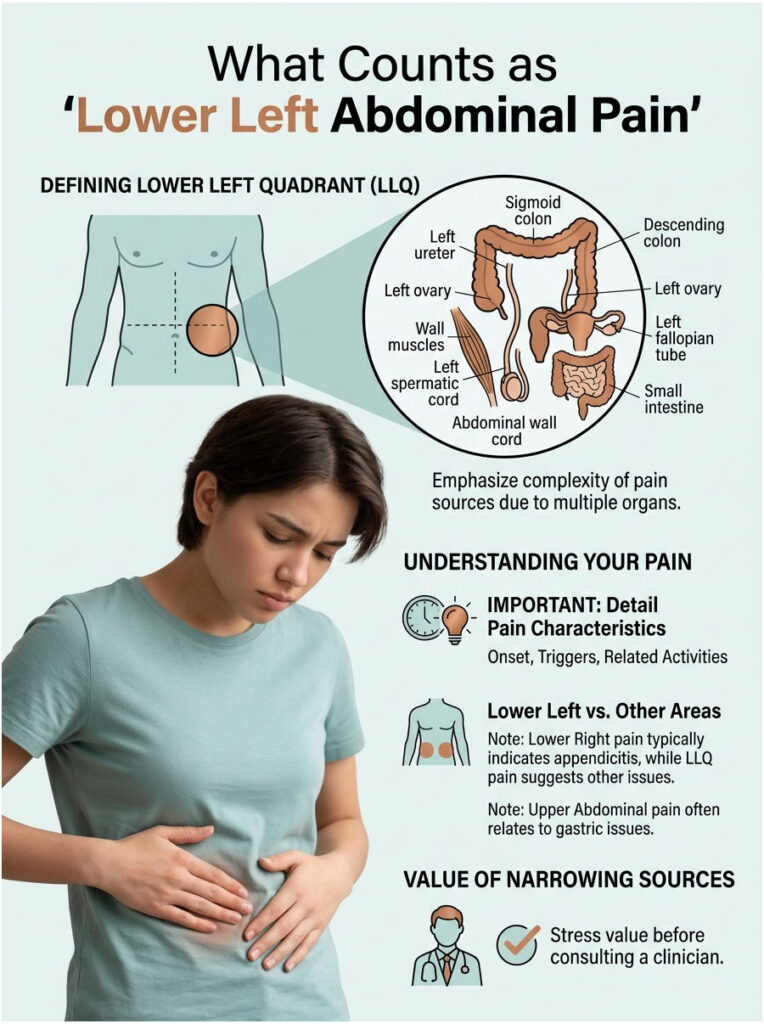
The region is densely packed. You have the sigmoid colon (the S-shaped final stretch of your large intestine before the rectum), part of your descending colon, the left ureter carrying urine from kidney to bladder, the left ovary and fallopian tube in women, the left spermatic cord in men, abdominal wall muscles, and a small portion of small intestine.
Because so many organs share this space, the same dull ache can spring from completely different systems. That is why a careful read of the pain pattern matters before you guess.
Our medical reviewers note that patients booking imaging tests with HealthCareOnTime often describe the pain differently across visits, which slows diagnosis. Jotting down when it started, what makes it worse, and what you ate or did before it began saves your doctor real time.
How Pain Here Differs From Other Abdominal Pain
Lower right pain points the finger at your appendix first. Lower left pain usually does not, because your appendix sits on the right. Upper-belly pain leans gastric (stomach, gallbladder, pancreas). Midline pain can mean small intestine or aorta.
Pain in the lower left section, by contrast, tends to follow the sigmoid colon or the urinary or reproductive tracts. That alone narrows the suspect list before you ever see a clinician.
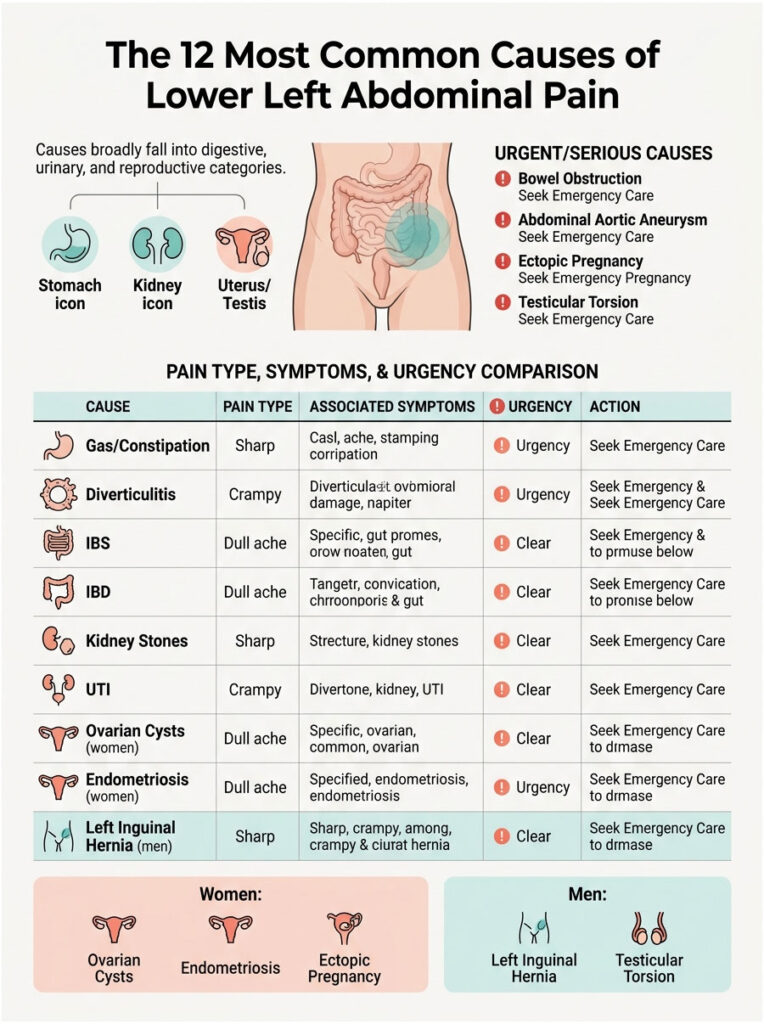
The 12 Most Common Causes of Lower Left Abdominal Pain
Most cases trace back to one of three buckets: digestive, urinary, or reproductive. Some are minor and self-limiting. Others need same-day care.
Digestive Causes
Gas and bloating top the list for sheer frequency. Trapped intestinal gas stretches the colon wall and creates sharp, shifting pain that often eases after passing gas or stool. Most cases clear on their own within a few hours.
Constipation causes a heavy, dull, cramping ache where stool collects in the sigmoid colon before exiting. You may feel a firm lump when you press on the area. Fiber, water, and movement usually sort it out.
Diverticulitis is the headline diagnosis for adults over 40 with persistent left-sided pain. Small pouches called diverticula form in the colon wall, most often in the sigmoid section, and one becomes inflamed or infected. According to the NIDDK, about 200,000 Americans are hospitalized for diverticulitis each year, and the condition drives roughly 450,000 emergency department visits annually.
Irritable bowel syndrome (IBS) affects roughly 6% of US adults under Rome IV criteria, with women diagnosed twice as often as men. Pain is crampy, comes and goes, and links tightly to bowel-habit changes (diarrhea, constipation, or both alternating). Bloating, gas, and mucus in stool round out the picture.
Inflammatory bowel disease (IBD), including ulcerative colitis and Crohn’s disease, brings left-sided cramping with bloody diarrhea, weight loss, and fatigue. IBD is far less common than IBS but far more serious, affecting around 1.3 million Americans per CDC estimates.
Colitis from infection or reduced blood flow can produce sudden left-sided pain plus diarrhea, sometimes bloody. Ischemic colitis most often hits adults over 60 with cardiovascular risk factors.
Urinary Causes
Kidney stones on the left side produce some of the most intense pain in medicine. Many patients describe it as worse than childbirth. The pain comes in waves, starts in the back or flank, and radiates down into the lower abdomen and groin. NHANES data show that about 11% of US adults have had a kidney stone in their lifetime.
Urinary tract infections (UTIs) can push pain into the lower abdomen, especially when the infection reaches the bladder or left kidney (pyelonephritis). Burning urination, urgency, cloudy urine, and low-grade fever are the giveaways.
Reproductive Causes (Women)
Ovarian cysts on the left ovary can produce a dull ache or sharp twinge depending on size and whether they rupture. A ruptured cyst causes sudden, severe pain and may need urgent imaging.
Endometriosis affects an estimated 11% of US women of reproductive age, according to the Office on Women’s Health. Pain often worsens around menstruation and can be sharp, deep, and persistent.
Ectopic pregnancy is a medical emergency. A fertilized egg implants outside the uterus, often in a fallopian tube, and as it grows, it causes sharp lower abdominal pain that can localize to either side. Light vaginal bleeding, shoulder-tip pain, and dizziness in a sexually active person of reproductive age means ER immediately.
Pelvic inflammatory disease (PID) from untreated chlamydia or gonorrhea brings lower abdominal pain, fever, abnormal discharge, and pain during intercourse. The CDC reports more than 770,000 American women receive PID treatment each year.
Reproductive and Groin Causes (Men)
Left inguinal hernia happens when part of the intestine pushes through a weak spot in the abdominal wall near the groin. It often shows up as a visible bulge and worsens with lifting, coughing, or straining.
Left testicular torsion is a surgical emergency. The spermatic cord twists and cuts off blood supply to the testicle, causing sudden, severe pain that can radiate up into the lower abdomen. Without surgery within 6 hours, the testicle can be lost.
Vascular and Rare Causes
Abdominal aortic aneurysm (AAA), psoas abscess, retroperitoneal hemorrhage, and bowel obstruction sit at the rare end of the list but carry high stakes. Sudden severe pain with low blood pressure or a pulsating sensation in the belly is a 911 situation.
Table 1: Core Comparison of the 12 Most Common Causes
| Cause | Typical Pain Type | Associated Symptoms | Urgency | First-Line Action |
| Gas / bloating | Sharp, shifting | Belching, relief after passing gas | Low | Walk, peppermint tea, OTC simethicone |
| Constipation | Dull, heavy, crampy | Hard stool, straining, fullness | Low | Fiber, water, mild laxative |
| Diverticulitis | Steady, sharp, localized | Fever, nausea, bowel-habit change | High | Same-day doctor or ER; CT scan |
| IBS | Crampy, comes and goes | Bloating, alternating diarrhea/constipation | Low-Med | Diet log, gastroenterologist referral |
| IBD (UC, Crohn’s) | Crampy, persistent | Bloody diarrhea, weight loss, fatigue | High | GI specialist; colonoscopy |
| Kidney stones | Severe waves, radiates to groin | Blood in urine, nausea, restlessness | High | ER for pain control and imaging |
| UTI / pyelonephritis | Burning + dull ache | Frequency, urgency, fever | Med-High | Urgent care; urinalysis, antibiotics |
| Ovarian cyst (women) | Dull or sharp twinge | Cycle-linked, bloating | Low-High | Pelvic ultrasound |
| Endometriosis (women) | Deep, cycle-linked | Heavy periods, painful sex | Med | OB-GYN evaluation |
| Ectopic pregnancy (women) | Sharp, worsening | Missed period, light bleeding, dizziness | Emergency | ER immediately |
| Inguinal hernia (men) | Pulling, bulge | Visible lump, worse with strain | Med | Surgical consult |
| Testicular torsion (men) | Sudden, severe | Swollen tender testicle, nausea | Emergency | ER within 6 hours |
How the Pain Feels: Sharp, Dull, Cramping, or Burning
The character of the pain is one of the strongest clues clinicians use. A sharp, stabbing sensation often points to inflammation, infection, or organ stretching. A dull constant ache leans toward chronic conditions or muscle strain. Crampy wave-like pain almost always involves the intestines or ureter.
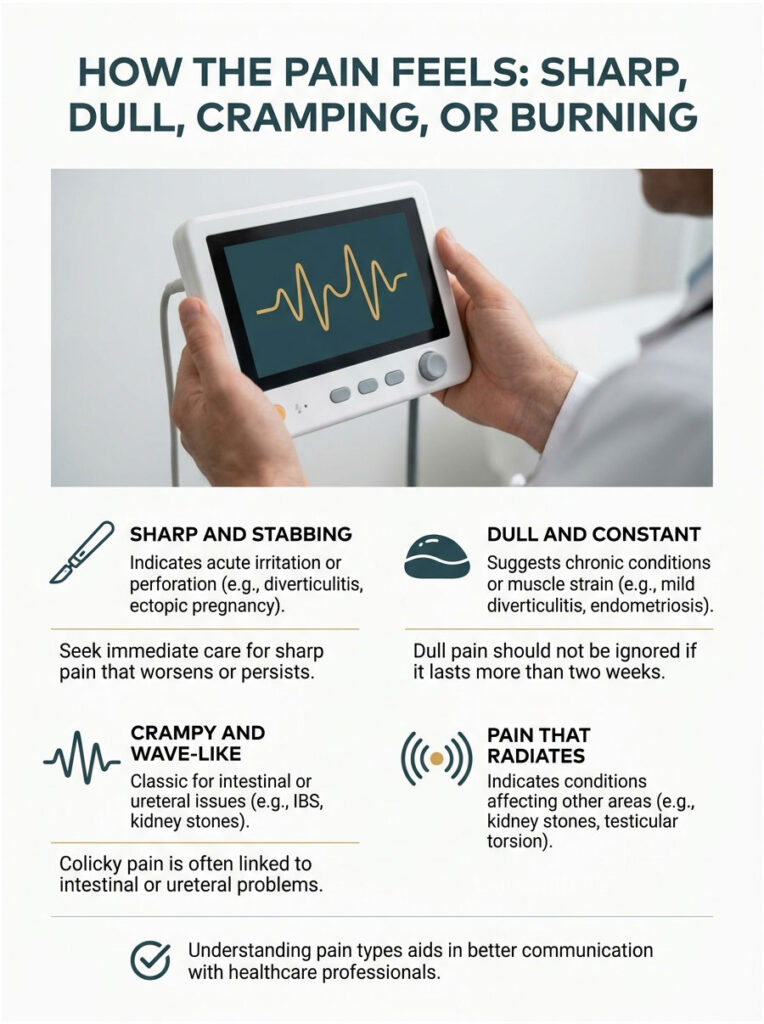
Sharp and Stabbing
Sharp pain that arrives suddenly and stays put usually means something is acutely irritated, perforated, or twisting. Diverticulitis, ovarian cyst rupture, ectopic pregnancy, testicular torsion, and a perforated bowel all live in this group.
If sharp pain stops you in your tracks, makes you guard the area, or builds over hours rather than fading, do not wait it out on the couch.
Dull and Constant
A dull, low-grade ache that has lingered for days or weeks points more toward chronic inflammation, slow processes, or muscle strain. Mild diverticulitis, endometriosis, unruptured ovarian cysts, and chronic constipation often show up this way.
Dull pain is easier to ignore but should not be brushed off if it persists beyond two weeks or starts to climb in intensity.
Crampy and Wave-Like
Crampy pain that comes in waves and eases between episodes (clinicians call it colicky pain) is classic for the intestines or the ureter. Bowel cramps from IBS, gas, or partial obstruction wax and wane. Kidney stone pain comes in dramatic surges as the stone moves down the ureter.
In cases reviewed across our diagnostic network, colicky lower-left pain that radiates into the groin or low back has a high pre-test probability of being a left ureteric stone.
Pain That Radiates
Pain that begins on the lower left and travels elsewhere tells its own story. Radiation to the back and groin suggests kidney stones. Radiation to the shoulder tip in a woman of reproductive age can mean internal bleeding (ectopic pregnancy or ruptured cyst). Radiation into the scrotum in men can mean testicular torsion or hernia.
Lower Left Abdominal Pain in Women vs Men
The organs in the lower left differ between sexes, so the most likely causes differ too. Mixing them up wastes precious time.
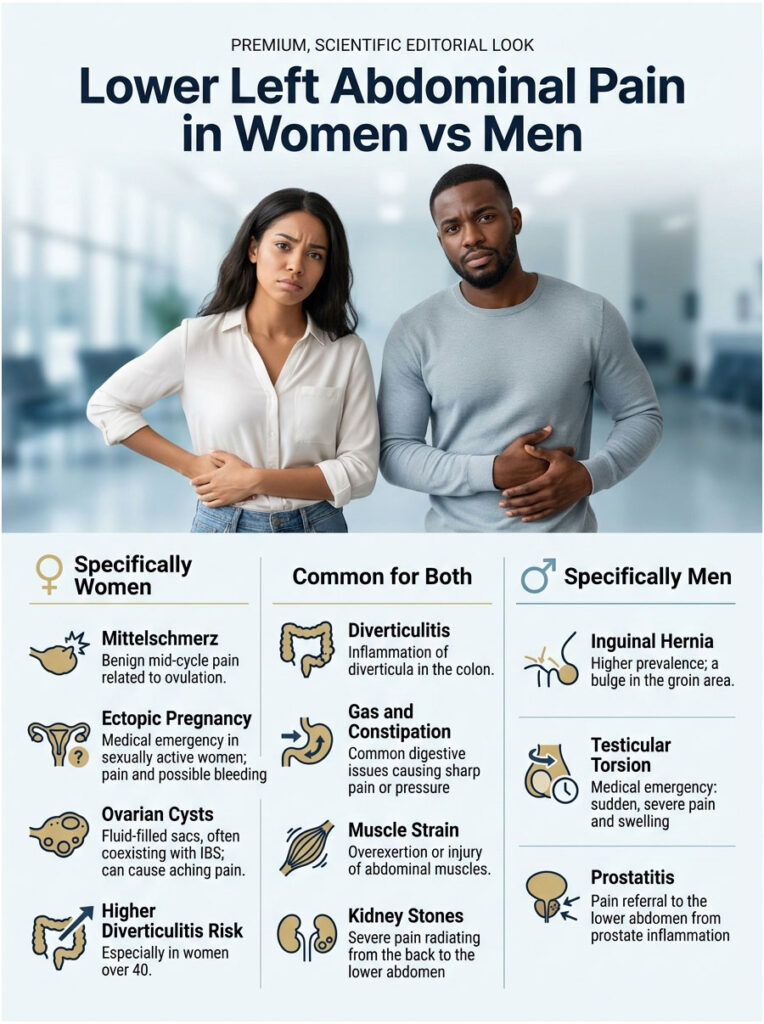
Patterns Specific to Women
Cycle timing matters. Mid-cycle pain (around day 14 of a 28-day cycle) often means mittelschmerz, the German word for ovulation pain, which is usually harmless. Pain in the days before or during menstruation can flag endometriosis or adenomyosis.
Pregnancy changes the rules. Any sexually active woman of reproductive age with new lower abdominal pain should be considered for ectopic pregnancy until proven otherwise, especially if periods have been irregular or missed.
Perimenopausal and postmenopausal women face higher rates of ovarian masses and diverticulitis. Per Gastro Hep Advances data published in 2023, women over 40 in the US have nearly twice the diverticulitis prevalence of men (228 vs 118 per 100,000).
Patients commonly ask our reviewers whether ovarian cysts and IBS can coexist, and the honest answer is yes. That overlap is one big reason a proper workup beats guessing.
Patterns Specific to Men
Inguinal hernias are about nine times more common in men than women, according to the American College of Surgeons. A new bulge in the left groin that shrinks when you lie down, paired with a pulling discomfort, is a hernia until proven otherwise.
Testicular torsion most often strikes adolescents and young men under 25 but can happen at any age. Sudden severe testicular pain with nausea, sometimes referred up into the lower abdomen, demands an ER visit within hours, not “first thing tomorrow.”
Prostatitis and prostate-related conditions can occasionally refer pain to the lower left abdomen, though midline or low-back pain is the more typical pattern.
Table 2: US Prevalence and Statistics by Condition
| Condition | US Prevalence / Annual Burden | Source |
| Abdominal pain ED visits (any cause) | ~9.46 million per year | NHAMCS / Academic Emergency Medicine 2024 |
| Diverticulosis (ages 50–59) | More than 30% of US adults | NIDDK |
| Diverticulitis hospitalizations | ~200,000 per year ($2.2B cost) | NIDDK / StatPearls |
| Diverticulitis ED visits | ~450,000 per year | Gastro Hep Advances 2023 |
| Kidney stones (lifetime) | 11% of US adults | NHANES 2015–2018 |
| IBS (Rome IV criteria) | 6.1% of US adults | Cedars-Sinai / Gastroenterology 2022 |
| Inflammatory bowel disease | ~1.3 million Americans | CDC |
| Endometriosis (women 15–44) | About 11% of US women | Office on Women’s Health |
Red Flags: When Lower Left Abdominal Pain Is an Emergency
Not every twinge needs a doctor, but certain symptom combinations are non-negotiable. The faster you act on red flags, the better the outcome, especially for diverticular perforation, ectopic pregnancy, and testicular torsion.
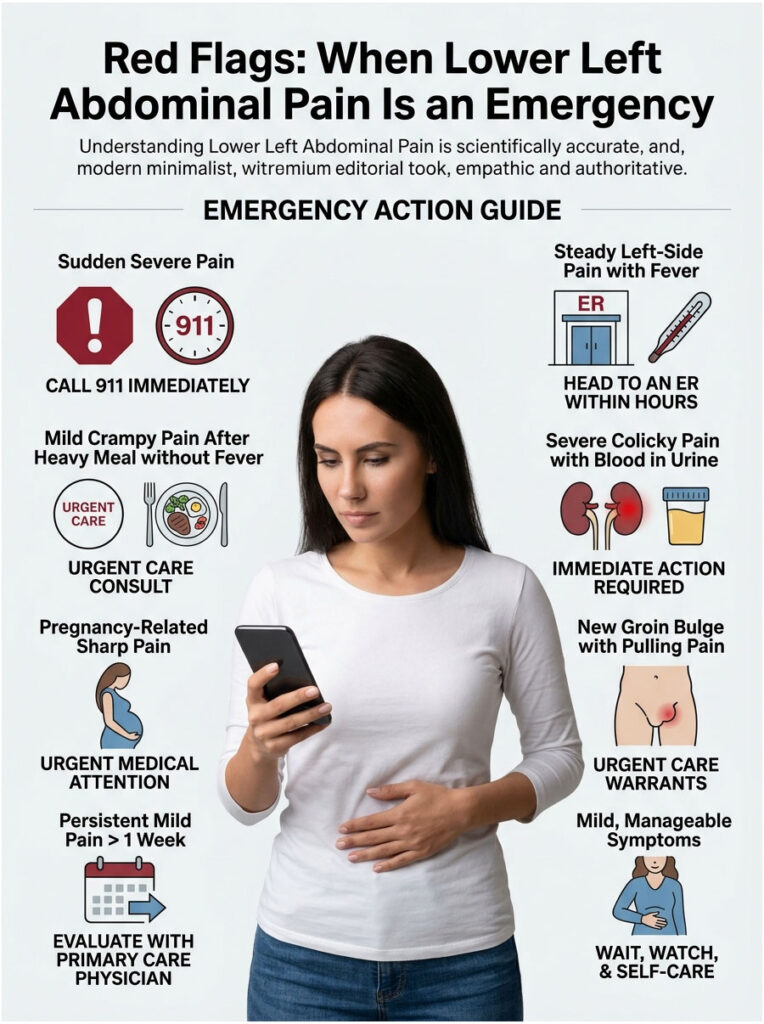
Call 911 Immediately
Sudden severe pain with any of these needs an ambulance, not a car ride:
- Rigid, board-like abdomen that hurts to touch anywhere
- Fainting or near-fainting
- Chest pain or shortness of breath alongside belly pain
- Vomiting blood or passing large amounts of black tarry or bright red stool
- Pulsating sensation in the abdomen with low blood pressure
- A pregnant woman with sharp one-sided pain and dizziness
Head to an ER Within Hours
Drive yourself (or get a ride) to an ER promptly for:
- Fever above 101°F (38.3°C) plus localized lower-left pain
- Pain so severe you cannot stand up straight
- Persistent vomiting that prevents keeping fluids down
- Suspected testicular torsion (severe testicular pain, swollen testicle)
- Suspected ectopic pregnancy (missed period, sharp pain, light bleeding)
- Bloody diarrhea with cramping that started suddenly
Urgent Care or Same-Day Doctor
For symptoms in this band, urgent care or a same-day primary care visit usually does the job:
- Steady localized pain for more than 24 hours without fever
- Pain plus burning urination or visible blood in urine
- New pain plus a noticeable groin bulge
- Worsening cramps with diarrhea that is not bloody
Wait, Watch, and Self-Care
Most gas, mild constipation, and short-lived crampy episodes settle at home. Wait-and-watch is reasonable if pain is mild, you can eat and drink, you are passing gas and stool, you have no fever, and you can pinpoint a plausible trigger (heavy meal, lactose, stress).
Table 3: Decision and Action Reference
| Your Scenario | Recommended Action | Timeframe |
| Mild crampy pain after a heavy meal, no fever | Walk, hydrate, OTC simethicone or antacid | Self-monitor 4 to 6 hours |
| Steady left-side pain, fever 100 to 101°F, nausea | Same-day primary care or urgent care | Within 12 hours |
| Sharp constant pain + fever above 101°F | ER for CT scan; possible diverticulitis | Same day |
| Severe colicky pain radiating to groin + blood in urine | ER for kidney stone evaluation | Immediate |
| Pregnant or possibly pregnant + sharp one-sided pain | Call 911 or go to ER | Immediate |
| New groin bulge + lower left pulling pain | Urgent care or surgeon | Within 24 to 48 hours |
| Severe testicular pain + lower abdominal pain | ER (testicular torsion suspected) | Within 6 hours |
| Pain lasting more than 1 week, mild but persistent | Primary care + possible GI referral | Within 1 to 2 weeks |
How Doctors Diagnose Lower Left Abdominal Pain
Diagnosis usually moves through three layers: hands-on exam, blood and urine work, and imaging. Knowing what each step adds helps you ask sharper questions when you are in the chair.

The Physical Exam
A clinician will press on different abdominal quadrants and watch for guarding (muscles tensing) and rebound tenderness (pain when pressure is released). They will check for a palpable mass in the lower left, signs of hernia in the groin, and bowel sounds with a stethoscope.
For women, a pelvic exam may follow. For men, a genitourinary check assesses hernia, testicular position, and tenderness.
Lab Tests
A standard workup typically includes:
- Complete blood count (CBC) to flag infection or bleeding
- C-reactive protein (CRP) to gauge inflammation severity
- Urinalysis to look for blood, infection, or stone fragments
- Beta-hCG pregnancy test for any reproductive-age woman
- Lipase if pancreatitis is on the differential
- Basic metabolic panel to assess kidney function and hydration
In tests booked through HealthCareOnTime, the CBC plus CRP combination flags inflammatory causes earliest, often before imaging makes a clear call.
Imaging
CT scan of the abdomen and pelvis with IV contrast is the workhorse for diagnosing diverticulitis, kidney stones, abscess, bowel obstruction, and many vascular causes. According to a 2024 Academic Emergency Medicine analysis, CT use for ED abdominal pain visits has more than doubled since 2007.
Ultrasound takes the lead for pregnant women, for ovarian and testicular evaluation, and for kidney imaging when radiation exposure is a concern. X-rays play a smaller role today but still help when bowel obstruction or free air is suspected.
Specialist Referrals
Depending on the suspected cause, your primary doctor may refer you to a gastroenterologist (for diverticulitis, IBS, IBD), urologist (kidney stones, recurrent UTIs), OB-GYN (ovarian, endometrial, pregnancy-related), or general surgeon (hernia, suspected appendicitis in an atypical left-sided presentation).
Treatment Approaches by Cause
Treatment depends entirely on the diagnosis. Self-treating without one is gambling, especially over age 40 when diverticulitis becomes common.
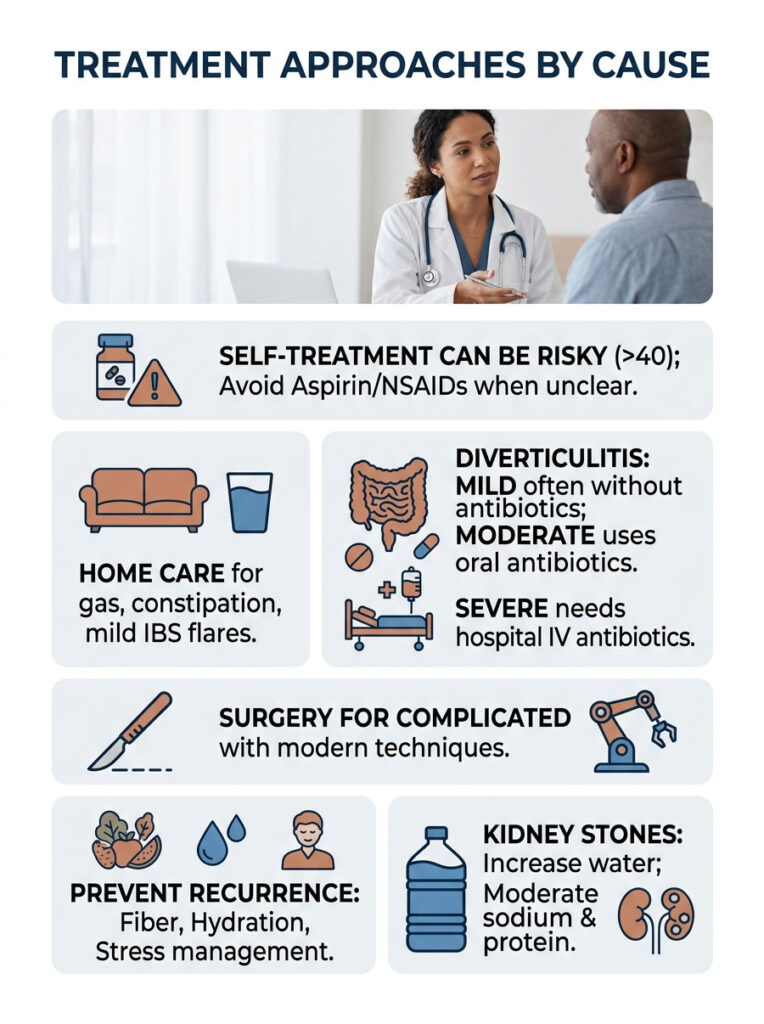
Home Care That Actually Helps
For uncomplicated gas, constipation, or mild IBS flares, evidence supports:
- Warm compress on the lower abdomen
- A 15 to 20 minute walk after meals
- Hydration: at least 64 ounces (about 2 liters) of water daily
- A heating pad set on low for 15 minute intervals
- OTC simethicone for gas, polyethylene glycol or psyllium for constipation
- Peppermint oil capsules for IBS cramps (with doctor approval)
Skip aspirin and NSAIDs (ibuprofen, naproxen) when the cause is unclear. Both can mask serious infection and worsen bleeding from diverticular or peptic disease.
When Antibiotics Are Appropriate
Uncomplicated mild diverticulitis in otherwise healthy adults is now often managed without antibiotics, per updated American Gastroenterological Association guidance. Moderate cases get oral antibiotics like ciprofloxacin plus metronidazole. Severe or complicated cases need IV antibiotics in the hospital.
UTIs almost always get antibiotics matched to a urine culture. Self-prescribing leftover antibiotics is one of the fastest ways to drive antibiotic resistance and complicate future treatment.
When Surgery Becomes Necessary
Surgery enters the picture for:
- Perforated diverticulitis or large abscess
- Recurrent severe diverticulitis episodes
- Bowel obstruction or stricture
- Testicular torsion (within hours)
- Strangulated hernia
- Ectopic pregnancy (if not amenable to medical management)
- Large, complex, or twisted ovarian cysts
Modern laparoscopic and minimally invasive approaches mean shorter hospital stays and faster recovery than open surgery offered 20 years ago.
Lifestyle Changes That Prevent Recurrence
For diverticular and IBS-related causes, the prevention playbook is consistent: aim for 25 to 38 grams of fiber daily (USDA recommendation), stay well-hydrated, move daily, limit ultra-processed foods, and manage stress with sleep, exercise, or therapy as needed.
For kidney stones, the single highest-yield change is drinking more water. Aim for urine output of at least 2.5 liters daily. Trimming sodium and animal protein, plus adequate dietary calcium, also helps for the most common stone types.
How to Prevent Lower Left Abdominal Pain (Evidence-Based)
You cannot prevent every cause, but you can shrink your risk for the most common ones with daily habits backed by US clinical guidelines.

Fiber, Fluids, and Gut Motility
The Dietary Guidelines for Americans recommend 25 to 38 grams of fiber per day depending on age and sex. Most Americans get half that. A high-fiber diet lowers diverticulitis risk, supports healthy bowel movements, and reduces constipation-related left-side pain.
Pair fiber with at least 64 ounces of water daily. Fiber without fluid can actually make constipation worse, a point our nutrition reviewers see surprise patients again and again.
Hydration and Kidney Stone Prevention
Adequate hydration is the cheapest insurance policy against kidney stones. Lemon water adds citrate, which inhibits stone formation. Cutting back on sugary drinks, especially colas, lowers risk further.
If you have already had one stone, your chance of another within 10 years is roughly 50%. Annual urinalysis and 24-hour urine testing help guide a personalized prevention plan.
Stress, Sleep, and the Gut-Brain Connection
IBS, functional abdominal pain, and stress-driven gut symptoms respond meaningfully to sleep, exercise, and mind-body therapies. Cognitive behavioral therapy and gut-directed hypnotherapy both have strong evidence for IBS.
In cases reviewed across our diagnostic network, patients who track stress alongside symptoms identify their personal triggers faster than those who only track food.
Frequently Asked Questions
What organ is in the lower left abdomen?
The lower left abdomen houses the sigmoid colon (the S-shaped end of the large intestine), part of the descending colon, the left ureter, the left ovary and fallopian tube in women, and the left spermatic cord structures in men. Abdominal wall muscles and a portion of small intestine also pass through this region.
When should I worry about lower left abdominal pain?
Worry and act fast if pain is sudden and severe, lasts longer than 48 hours without improvement, or comes with fever above 101°F, persistent vomiting, blood in stool or urine, fainting, a rigid abdomen, or suspicion of pregnancy. Mild crampy pain that improves within a day, with no other symptoms, is rarely dangerous.
Can gas alone cause severe lower left abdominal pain?
Yes. Trapped gas in the sigmoid colon can produce sharp stabbing pain intense enough to send people to the ER. The difference from serious causes is that gas pain shifts location, eases with movement or passing gas, and clears within hours. Gas does not cause fever, bloody stools, or guarding.
How do I know if it’s diverticulitis vs IBS?
Diverticulitis usually brings localized constant lower-left pain plus fever, nausea, and often elevated white blood cells on a CBC. IBS pain is crampy, comes and goes for months or years, ties closely to bowel movements, and does not cause fever or weight loss. CT imaging and lab work distinguish them definitively.
Is lower left abdominal pain a sign of colon cancer?
Colon cancer can cause lower left pain, especially if a tumor sits in the sigmoid or descending colon, but it is far from the most common cause. Red flags pointing toward malignancy include unexplained weight loss, persistent change in bowel habits beyond 6 weeks, anemia, and visible blood in stool. The US Preventive Services Task Force recommends colonoscopy screening starting at age 45.
Why does it hurt more when I press on it?
Tenderness to direct pressure (called point tenderness) suggests an inflamed organ or tissue sits just under the skin. Rebound tenderness (pain when pressure is released) is more concerning and can indicate peritoneal irritation from infection or perforation. Both findings push clinicians toward urgent imaging.
Can stress cause lower left abdominal pain?
Yes, indirectly. Stress activates the gut-brain axis and worsens IBS, functional abdominal pain, and acid reflux. It does not cause structural problems like diverticulitis or kidney stones, but it can amplify how intensely you feel pain from any cause. Chronic stress is linked to higher rates of IBS flare-ups in US studies.
How long should I wait before seeing a doctor?
For mild new pain with no red flags, 24 to 48 hours of self-monitoring is reasonable. If pain persists beyond 2 days, worsens at any point, or develops new symptoms (fever, bleeding, vomiting), schedule a same-day visit. Severe pain or any red flag means same-day medical evaluation, not waiting.
What does kidney stone pain feel like on the left side?
A left kidney stone produces severe colicky pain that starts in the left flank or back and radiates downward into the lower left abdomen and groin. The pain comes in waves lasting 20 to 60 minutes, often with nausea, vomiting, restlessness (people cannot sit still), and sometimes pink, red, or brown urine.
Can ovulation cause left-sided pain?
Yes. Mittelschmerz, the German word for ovulation pain, affects roughly 1 in 5 women. It produces mild sharp or crampy pain on one side of the lower abdomen, lasting minutes to a couple of days, around day 14 of a 28-day cycle. It alternates sides month to month and needs no treatment beyond comfort care.
Does diverticulitis go away on its own?
Mild uncomplicated diverticulitis can resolve with bowel rest, a clear liquid diet, and time, especially in otherwise healthy adults. Many cases still benefit from antibiotics and follow-up imaging. Complicated diverticulitis with abscess, perforation, or obstruction never resolves on its own and needs hospital care.
What tests should I ask my doctor to order?
For unexplained persistent lower-left pain, reasonable starting tests include a CBC, CRP, urinalysis, basic metabolic panel, and pregnancy test (for women of reproductive age). If the workup suggests structural disease, a CT scan of the abdomen and pelvis or pelvic ultrasound usually follows. A gastroenterology or urology referral may come next.
Disclaimer: This article is for general health information only and is not a substitute for diagnosis or treatment by a licensed US healthcare professional. Lower left abdominal pain has many possible causes, some of which are medical emergencies. If your symptoms match any red flags described above, contact 911 or visit your nearest emergency department immediately. HealthCareOnTime does not provide direct medical care for US patients and recommends consulting your physician for personal evaluation.
References
- National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). Definition & Facts for Diverticular Disease — https://www.niddk.nih.gov/health-information/digestive-diseases/diverticulosis-diverticulitis/definition-facts
- Wu et al. Trends in ED abdominal pain visits, imaging, and diagnosis 2007–2019. Academic Emergency Medicine, 2024 — https://onlinelibrary.wiley.com/doi/10.1111/acem.15017
- Cleveland Clinic. Lower Abdominal Pain: Causes & Treatment — https://my.clevelandclinic.org/health/symptoms/24530-lower-abdominal-pain
- Cedars-Sinai. Prevalence of IBS Exceeds Previous Estimates — https://www.cedars-sinai.org/newsroom/study-prevalence-of-ibs-exceeds-previous-estimates/
- StatPearls / NCBI. Diverticulitis — https://www.ncbi.nlm.nih.gov/books/NBK541110/
- Gastro Hep Advances. Sex, Race, and Ethnicity Differences in Diverticular Disease ED Presentations — https://www.ghadvances.org/article/S2772-5723(23)00187-5/fulltext
- NHANES via Incidence of Kidney Stones in the US — https://pubmed.ncbi.nlm.nih.gov/34854755/
- CDC. Inflammatory Bowel Disease Data and Statistics — https://www.cdc.gov/ibd/data-statistics.html
- Office on Women’s Health. Endometriosis — https://www.womenshealth.gov/a-z-topics/endometriosis
- American Gastroenterological Association. IBS in America 2024 Survey — https://gastro.org/press-releases/ibs-in-america-despite-advances-ibs-remains-a-burden-for-many-millions/
- Medical News Today. What’s causing pain in my lower left abdomen? — https://www.medicalnewstoday.com/articles/320069
- Healthline. Pain in Lower Left Abdomen — https://www.healthline.com/health/pain-in-lower-left-abdomen





