

Here is a truth that surprises most new parents: in the majority of babies, spitting up is a laundry problem, not a medical one. The real skill is learning the small set of signs that flip it from normal to “call your pediatrician.”
Table of Contents
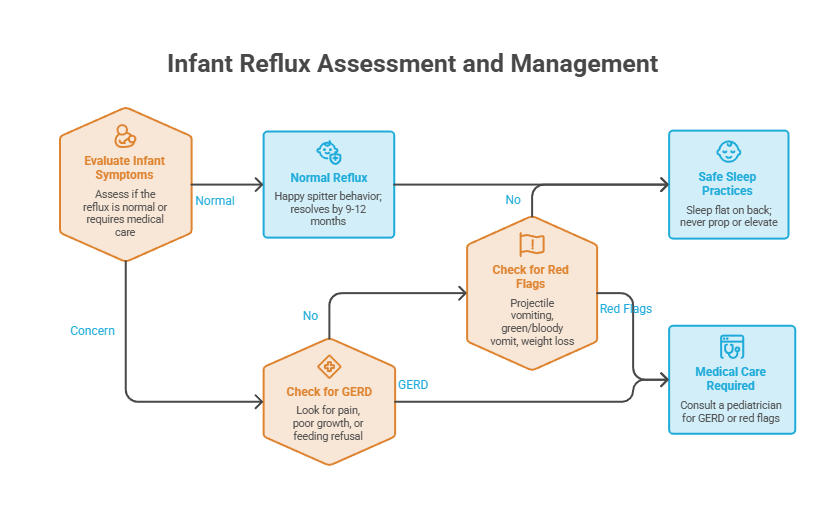
Quick Answer: Acid reflux in infants, called gastroesophageal reflux (GER), is when stomach contents flow back up into the esophagus and cause spit-up. It’s normal for most healthy babies, starts around 2 to 3 weeks, peaks near 4 months, and fades by about 12 months. When reflux causes pain, poor weight gain, or other complications, it’s called GERD and needs a pediatrician.
At a Glance
- Most infant reflux is normal “happy spitter” behavior that resolves on its own.
- Reflux usually starts at 2 to 3 weeks, peaks around 4 months, and clears by 9 to 12 months.
- The cause is a still-developing muscle valve plus a liquid diet and lots of lying down.
- GERD is different: it involves pain, poor growth, or feeding refusal and needs medical care.
- Red flags like projectile vomiting, green or bloody vomit, or weight loss warrant a prompt call.
- For reflux, babies should still sleep flat on their backs; never prop or elevate the crib.
What Is Acid Reflux in Infants?
Acid reflux is one of the most common reasons worried parents reach out about their newborns. The good news is that the mechanics are simple, and so is the reassurance behind them.
What Reflux Is and Why Babies Spit Up
Reflux happens when food and liquid from your baby’s stomach travel back up into the esophagus, the tube connecting the mouth and stomach. That backward flow is what lands on your shoulder as spit-up.
The medical name is gastroesophageal reflux, or GER. According to the Cleveland Clinic, it’s usually harmless and happens because a baby’s digestive tract isn’t fully mature yet.
Parents of newborns we work with are often surprised by how normal daily spit-up actually is. For most babies, it’s a passing stage tied to growth, not a sign that anything is wrong.
To put it in perspective, spitting up is nearly universal in the early months. Most healthy babies do it, and for the majority it never causes a single health problem. Knowing that ahead of time can save a lot of unnecessary worry during those first messy weeks.
The Immature Lower Esophageal Sphincter, the Real Cause
At the bottom of the esophagus sits a ring-shaped muscle called the lower esophageal sphincter. It’s supposed to relax to let food into the stomach, then tighten to keep it there.
In babies, that valve is still developing. Like all of a baby’s muscles, it may not stay shut as well as it will later, so food and acid can press on it and push it open when it shouldn’t.
A few normal facts of baby life make this worse. Infants drink an all-liquid diet, spend much of the day lying flat, and have small stomachs that fill quickly. Together, those factors make occasional backflow almost expected, and none of it reflects anything you did wrong as a parent.
Spitting Up vs Vomiting, the Key Difference
This distinction matters more than almost anything else, so it’s worth getting right. Spitting up means stomach contents flow easily out of the mouth, often with a burp, in small amounts, and without strong muscle contractions.
Vomiting is different. It involves forceful muscle contractions that push stomach contents out, usually with discomfort and crying. Spitting up typically doesn’t bother a baby at all.
Our medical reviewers note that the “does it bother the baby” test is one of the fastest ways to separate ordinary reflux from something that needs a closer look. A content baby who spits up is in a very different situation from one who vomits and cries hard.
One more reassuring detail: spit-up almost always looks like more than it is. A tablespoon of milk can spread across a whole onesie and seem like the entire feeding came back up. If your baby is feeding well and growing, the volume on your shirt is rarely the full story.
GER vs GERD: What’s Normal and What’s Not
Almost every parent question about reflux comes down to one line: is this normal, or is it the serious version? Here is the clean distinction, then how the two compare.
The “Happy Spitter” (Normal GER)
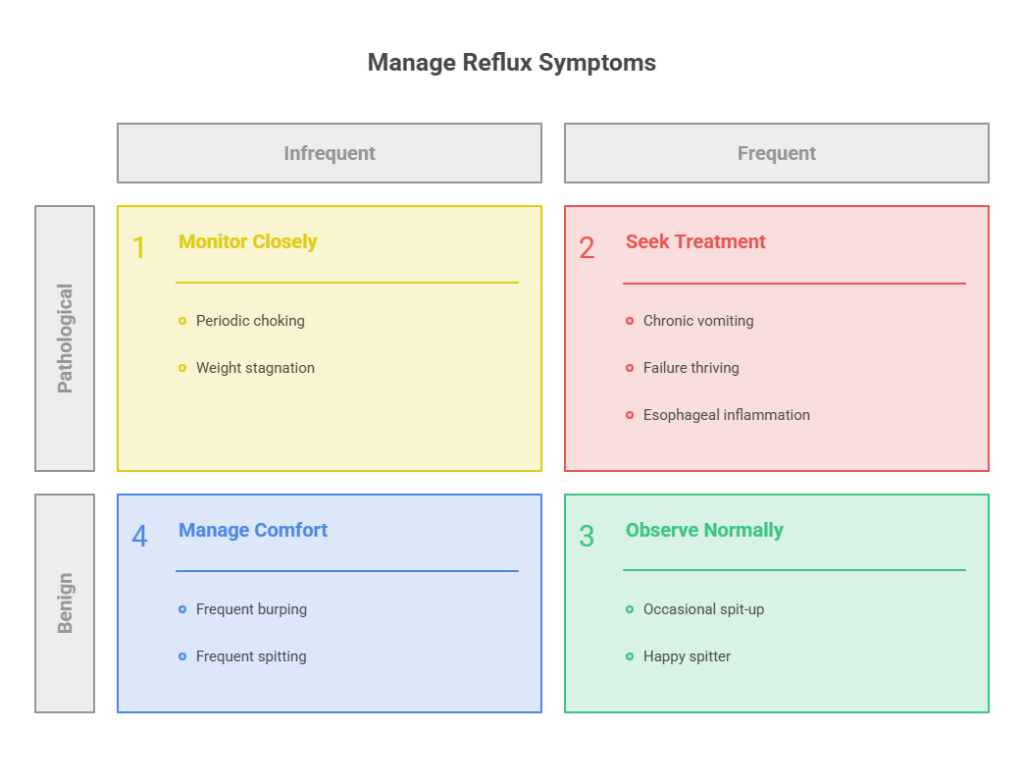
Plenty of babies spit up often, even daily, with zero health problems. Providers call these babies “happy spitters” because the spitting up doesn’t seem to bother them, and they may even feel better afterward.
A happy spitter keeps gaining weight, feeds well enough, and is generally comfortable. The spit-up is messy, but the baby is thriving, which is the reassuring picture you want to see.
When It Becomes GERD
In one line: GER is harmless spit-up, and GERD is reflux that hurts or harms. GERD is a more severe, longer-lasting condition in which reflux causes repeated bothersome symptoms or leads to complications.
The signs go beyond laundry. GERD often begins before 8 weeks of age and can include frequent or forceful spit-up or vomiting (six or more times a day), discomfort, and feeding difficulty.
Over time, GERD complications can include esophagitis (inflammation of the esophagus), poor weight gain, and problems outside the esophagus. Those are the reasons GERD earns a pediatrician’s attention rather than a wait-and-see approach.
GERD can also show up beyond the stomach. Some babies develop a chronic cough, wheezing, congestion, or hoarseness, and a few have frequent respiratory infections. These signs overlap with many other conditions, which is why a pediatrician’s assessment matters rather than self-diagnosis.
Which Babies Are More Likely to Have GERD
Any baby can develop GERD, but some carry higher risk. It’s more common in premature infants and in babies with conditions affecting the esophagus, nervous system, or lungs.
Cow’s milk protein allergy, neurologic impairment, and developmental delay also raise the frequency and severity of GERD. In cases reviewed across our network, prematurity and milk protein allergy are two of the patterns that most often turn simple spit-up into something more.
The table below sums up the difference parents most want to understand.
| What to Look At | GER (“Happy Spitter”) | GERD | Why It Matters |
| Spit-up pattern | Effortless, small, often with a burp | Frequent or forceful, 6+ times daily | Forceful or frequent vomiting is a warning sign |
| Baby’s comfort | Calm, content, often feels better after | Pain, crying, arching, irritability | Distress points toward GERD, not normal GER |
| Weight and growth | Steady, on the curve | Poor weight gain or weight loss | Growth is the single most telling clue |
| Feeding behavior | Feeds well, maybe occasional fuss | Refuses feeds, prolonged or interrupted | Feeding refusal signals a problem |
| Typical course | Fades by 9 to 12 months on its own | Persistent, may need medical treatment | GER rarely needs medicine; GERD may |
What Causes Infant Reflux (and When It Peaks)
Understanding why reflux happens, and when it tends to ease, takes a lot of the fear out of those early months. The timeline is remarkably predictable.
Normal Infant Physiology
The root cause is just immaturity. A baby’s all-liquid diet flows back up easily, the stomach is tiny and fills fast, and newborns spend most of their time horizontal, which gravity does not help.
Add the still-developing valve at the top of the stomach, and backflow becomes a normal byproduct of being a baby. This is biology, not a feeding mistake.
The Reflux Timeline: Onset, Peak, and Resolution
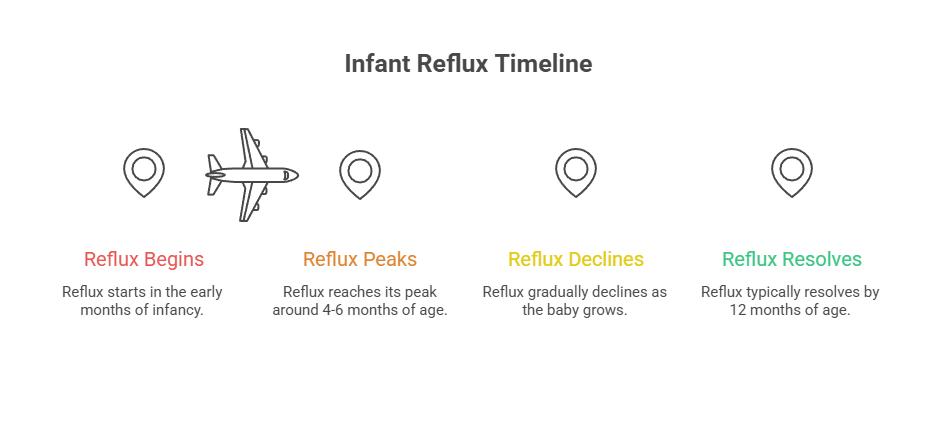
Reflux follows a clear arc. Infant reflux usually begins at 2 to 3 weeks, peaks at 4 to 5 months, and should fully resolve by 9 to 12 months.
That fade-out isn’t random. GER disappears as the upper digestive tract matures, and milestones like better head control, sitting up, and starting solids all help symptoms improve.
Timing also offers clues. It’s unusual for reflux to start in the first week of life or after a baby turns 6 months, and those cases may point to GERD or another condition. The same goes for symptoms that drag on well past the first birthday.
Risk Factors That Make Reflux More Likely
Beyond normal physiology, prematurity tops the list, since a preemie’s valve and digestive system have had less time to develop. Babies with neurologic conditions or certain anatomical differences are also more prone.
Cow’s milk protein allergy deserves special mention, because it can mimic or worsen reflux and sometimes responds to a feeding change. A family history of reflux may play a role too.
Here’s the picture in numbers, which is more reassuring than most parents expect.
| Statistic | Figure | Source |
| Infants with daily regurgitation by 2 months | 70 to 85 percent | NIDDK / NIH |
| Prevalence peak at 4 months | About two-thirds spit up daily | AAFP / NASPGHAN |
| Healthy infants who experience GER | Up to two-thirds | AAP, Pediatrics |
| Age most babies outgrow reflux | 12 to 14 months | NIDDK / NIH |
| Higher-risk groups | Premature, CMPA, neurologic conditions | NIDDK / AAP |
Those figures come from sources like the National Institute of Diabetes and Digestive and Kidney Diseases, which reports that 70 to 85 percent of infants have daily regurgitation by 2 months and most no longer have symptoms by 12 to 14 months. The American Academy of Family Physicians notes that regurgitation occurs at least once daily in half of infants up to 3 months, peaking at 4 months when two-thirds regurgitate daily.
A Word on Silent Reflux and the Crying Overlap
Not all reflux is visible. With “silent reflux,” stomach contents come up but the baby swallows them back down, so you see little or no spit-up while the baby may still seem uncomfortable.
Here’s the nuance newer research stresses: fussiness often gets blamed on reflux when the timing is really just coincidence. The peak age for reflux overlaps with normal developmental crying, so a crying baby may not be crying from acid at all.
That overlap is exactly why a careful pediatrician looks at the whole picture, growth, feeding, and comfort, rather than assuming every fussy spell is acid. It also explains why acid-reducing medicine so often fails to calm a crying baby.
When to Worry: Red Flags That Aren’t Just Reflux
This is the section every anxious parent skips ahead to read, and rightly so. Most spit-up is harmless, but a handful of signs should never be brushed off as “just reflux.”
Emergency Signs
A few symptoms call for fast medical attention. Red flags pointing to something other than reflux include forceful vomiting, vomit containing blood or bile, abdominal swelling, fever, and blood in the stools.
Green vomit is especially serious. Bilious (green) vomiting in an infant is a potential surgical emergency, because it can signal intestinal malrotation leading to a midgut volvulus.
Forceful, projectile vomiting is another. Repeated forceful vomiting should not be assumed to be reflux and needs evaluation for conditions like pyloric stenosis. Patients commonly ask us where the line is, and these are the signs our reviewers say should never wait.
Growth and Feeding Warning Signs
Growth is the quiet alarm bell. If your baby isn’t gaining weight as expected, is losing weight, or refuses to feed, that shifts the picture from normal reflux toward GERD or another issue.
Choking or gagging with the majority of feeds is also a flag that needs evaluation, as is projectile vomiting on top of spitting up. Persistent, excessive crying that nothing soothes belongs on this list too.
A simple frame helps: a baby who spits up but grows and feeds well is reassuring, while one whose growth or feeding falters needs a closer look from a pediatrician.
Other Conditions Reflux Can Mask
Reflux can resemble several other problems. Recurrent vomiting can occasionally mimic GERD due to a metabolic disease or an anatomical issue such as pyloric stenosis or malrotation.
There’s also Sandifer syndrome, a less common pattern. Some infants with reflux arch the back and turn the head to one side, which can look alarming but relates to the reflux itself. Cow’s milk protein allergy, often with a rash or diarrhea, is another mimic worth ruling out.
Timing matters here too. Recurrent vomiting or regurgitation beyond 18 months is uncommon and suggests GERD or more concerning pathology.
The action grid below turns these signs into a clear plan.
| What You Notice | Likely Meaning | What to Do |
| Forceful or projectile vomiting | Possible pyloric stenosis or other issue | Call your pediatrician promptly for evaluation |
| Green (bilious) or bloody vomit | Possible surgical emergency | Seek emergency care right away |
| Poor weight gain or feeding refusal | Possible GERD or another condition | Schedule a pediatrician visit soon |
| Choking, gagging, or arching with most feeds | Needs medical assessment | Call your pediatrician for an evaluation |
| Spits up but is happy and growing | Normal GER (happy spitter) | Reassurance; routine well-baby checks |
How to Help Your Baby’s Reflux at Home
For ordinary reflux, simple feeding and positioning tweaks do most of the work. These are the first steps pediatricians recommend before anything else.
Feeding Changes
Smaller, more frequent feedings keep the stomach from overfilling, which reduces backflow. Slowing the pace and burping your baby often during and after feeds helps too.
Avoiding overfeeding is one of the most effective changes. A stomach stretched past comfortable is far more likely to send milk back up.
Positioning While Awake
Keeping your baby upright for 20 to 30 minutes after feeds lets gravity do its job. Body position changes while awake are part of standard conservative care for infant reflux.
Supervised tummy time during awake hours supports development and core strength, which over months helps reflux improve. The key phrase is “while awake,” since sleep rules are different and stricter.
One caution: long stretches in a car seat, swing, or carrier can actually increase reflux by curling your baby forward and pressing on the stomach. Upright and supported is good; slumped and compressed is not. Use those seats for travel, not as all-day reflux fixes.
Thickened Feeds and Formula Changes
For some babies, thickening feeds helps. Options include a thickening agent such as rice cereal or an antiregurgitant (thickened) formula. These should be tried with your pediatrician’s guidance rather than improvised.
If a cow’s milk protein allergy is suspected, your pediatrician may suggest a formula change. Across patients we serve, a guided formula trial sometimes resolves what looked like stubborn reflux.
A Note for Breastfeeding Parents
Breastfeeding parents don’t need to stop. In some cases, a short trial of reducing certain foods in the parent’s diet, such as dairy, may help if a milk protein sensitivity is in play.
Our lab and clinical partners suggest making one change at a time and tracking the response, ideally with your pediatrician, so you can tell what’s actually working.
What to Avoid
A few common habits make reflux worse. Avoid overfeeding, tight diapers or waistbands that press on the belly, and bouncing or jostling your baby right after a feed. Cigarette smoke around your baby can worsen reflux too, so keep their space entirely smoke-free.
It also helps not to rush the next feeding. Giving the stomach a little time to settle, and keeping feeds calm and unhurried, tends to cut down on how much comes back up.
The Safe-Sleep Rule Every Reflux Parent Must Know
This is the single most important safety point in any reflux conversation, and our medical reviewers stress it above all others. Reflux does not change safe-sleep rules.
Why You Should Never Prop or Elevate the Crib
It’s tempting to tilt the mattress or use a wedge to “help” reflux. Resist that urge. Only supine (on the back) sleep positions can be recommended for infants, because the risk of sudden infant death syndrome is associated with all other sleeping positions.
Inclined sleepers, crib wedges, and positioners are not safe and are not recommended, even for babies with reflux. The reflux risk from flat sleeping is far smaller than the SIDS risk from unsafe positioning.
This advice has changed over the years, so older relatives may suggest propping or tummy sleeping for reflux. Those recommendations are outdated. Current guidance is clear that flat, back sleeping is safest, and it’s worth gently explaining that to well-meaning family.
Back to Sleep, Even With Reflux
The rule is steady: babies sleep on their backs, on a firm flat surface, with nothing extra in the crib. Healthy babies are well designed to protect their airway during sleep, even with some reflux.
If reflux feels severe enough that flat sleep seems impossible, that’s a reason to talk with your pediatrician, not a reason to prop the crib.
Should Your Baby Take Reflux Medication?
Many parents arrive expecting a prescription will fix things. For ordinary reflux, the current evidence points the other way, and that surprises a lot of families.
Why Acid Suppressants Usually Aren’t the Answer for GER
Acid-reducing drugs simply don’t target the problem in simple reflux. Acid suppressants such as H2 blockers and proton pump inhibitors reduce stomach acidity but are not effective against GER.
Part of the reason loops back to the crying overlap. If the fussiness isn’t from acid, reducing acid won’t calm it, which is what studies of treated babies have repeatedly found.
The Risks, and What the AAP Recommends
These medicines carry real downsides in babies. Acid suppressants have been linked to a higher risk of serious infections and fractures.
Weighing those risks against unclear benefit led to a clear stance. Choosing Wisely and the American Academy of Pediatrics recommend against the use of acid suppressants in infants with GER. Patients commonly ask us about reflux medicine, and this is the guidance our reviewers point to.
When Medication Is Appropriate
Medication still has a place for true GERD. For infants with GERD that doesn’t improve with conservative measures, an empiric four-week trial of acid suppression may be considered.
That decision belongs to your pediatrician, based on signs like poor weight gain or evidence of esophagitis, not on spit-up frequency alone. The default for a happy, growing spitter is patience, not a prescription.
What to Expect: The Reflux Timeline and Outlook
The outlook for infant reflux is genuinely encouraging, which is the note worried parents most need to hear. Time is on your side.
How Most Cases Resolve on Their Own
For the great majority of babies, reflux is a phase that ends without treatment. Most regurgitation resolves by 12 months of age and does not require treatment.
As your baby grows, sits upright, gains core strength, and starts solids, the spit-up tapers off. The messy months pass, and most families look back on them as a brief, normal chapter.
There’s also nothing you need to “cure” in a happy spitter. The goal isn’t to stop every spit-up, it’s to keep your baby comfortable and growing while time and development do the real work. That shift, from fixing to supporting, takes pressure off exhausted parents.
Tracking Progress and Partnering With Your Pediatrician
Routine well-baby visits are the best tool for peace of mind. Your pediatrician tracks weight and growth, the clearest sign that reflux is staying in the harmless lane.
In tests and visits coordinated through HealthCareOnTime, the same theme comes up: a baby who is growing and comfortable is almost always fine, even when the laundry pile says otherwise. Keep notes on feeding, spit-up, and mood to share at each visit.
A simple log goes a long way. Jot down feeding times and amounts, how often your baby spits up, any crying or arching, wet and dirty diapers, and weight at checkups. Patterns on paper help your pediatrician separate normal reflux from a problem far faster than memory alone.
Frequently Asked Questions
What is the difference between GER and GERD in infants?
GER is ordinary reflux, the harmless spitting up most babies do, and it resolves on its own. GERD is reflux that causes bothersome symptoms or complications, such as pain, poor weight gain, feeding refusal, or esophagitis. GERD needs a pediatrician’s evaluation, while simple GER usually does not.
How much spit-up is normal for a baby?
A lot, honestly. Up to two-thirds of healthy infants spit up regularly, and many do so daily, especially around 4 months. As long as your baby is comfortable and gaining weight well, frequent spit-up is typically normal. Forceful or six-plus-times-daily vomiting is worth discussing with your pediatrician.
When does infant reflux peak and when does it go away?
Reflux usually begins at 2 to 3 weeks of age and peaks around 4 to 5 months. For most full-term babies, it fades by 9 to 12 months as the digestive tract matures and the baby sits up and starts solids. Symptoms persisting past 18 months should be evaluated.
What’s the difference between spitting up and vomiting?
Spitting up is effortless, comes up in small amounts, often with a burp, and doesn’t bother your baby. Vomiting is forceful, driven by strong muscle contractions, and usually causes discomfort and crying. Spitting up is typically normal reflux, while frequent forceful vomiting deserves a closer look.
How do I know if my baby’s reflux is causing pain?
Watch your baby, not just the spit-up. Pain signs include crying or arching during or after feeds, irritability, and refusing to eat. A “happy spitter” who is calm and growing is likely fine. Persistent distress, especially with poor weight gain, suggests GERD and warrants a pediatrician visit.
Is it safe to elevate my baby’s crib or use a wedge for reflux?
No. Only flat, on-the-back sleep is recommended, because all other sleep positions and inclined or wedge products raise the risk of sudden infant death syndrome. Even with reflux, babies should sleep flat with nothing extra in the crib. Raise concerns with your pediatrician instead of propping the crib.
Should my baby take reflux medicine like a PPI?
Usually not for ordinary reflux. The AAP and Choosing Wisely recommend against acid suppressants for infants with simple GER, since the drugs don’t help typical spit-up and carry risks like infections and fractures. Medication may be appropriate for confirmed GERD, a decision your pediatrician makes.
Can formula or breast milk affect my baby’s reflux?
It can. Overfeeding and large, fast feeds tend to worsen reflux regardless of feeding method. For some babies, a cow’s milk protein sensitivity contributes, and a guided formula change or a parent’s short dairy-reduction trial may help. Make changes with your pediatrician rather than experimenting on your own.
What is silent reflux in babies?
Silent reflux is when stomach contents come back up but the baby swallows them instead of spitting up, so there’s little visible spit-up. It can still cause fussiness, swallowing or feeding issues, or discomfort. Because it’s harder to spot, mention any feeding distress to your pediatrician for proper assessment.
Can a cow’s milk allergy be mistaken for reflux?
Yes. Cow’s milk protein allergy can mimic or worsen reflux and may come with a rash, diarrhea, or blood in the stool. It’s more closely linked with GERD than simple GER. If your baby has these added signs, your pediatrician can evaluate for a milk protein allergy and suggest a feeding change.
Does tummy time or holding my baby upright help?
Holding your baby upright for about 20 to 30 minutes after feeds uses gravity to reduce backflow and often helps. Supervised tummy time while awake supports core strength and development over time. Both are awake-only strategies; for sleep, babies still go flat on their backs.
When should I call the doctor about my baby’s spit-up?
Call promptly for projectile vomiting, green or bloody vomit, poor weight gain, feeding refusal, choking or gagging with most feeds, fever, or a baby who seems in pain. Green or bloody vomit warrants emergency care. When something feels off, trust your instincts and check with your pediatrician.
Medical Disclaimer: This article is for general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Every baby is different, and reflux symptoms can overlap with other conditions. Always consult your pediatrician about your child’s specific situation. For emergency signs such as green or bloody vomit, breathing trouble, or signs of dehydration, seek emergency care or call 911 right away.
References
- NIDDK / NIH: Acid Reflux (GER & GERD) in Infants
- HealthyChildren.org (AAP): GER & GERD
- Mayo Clinic: Infant Acid Reflux, Symptoms and Causes
- Cleveland Clinic: Reflux in Babies, Signs & Treatment
- AAP, Pediatrics: Overuse of Reflux Medications in Infants
- AAFP: Diagnosis and Treatment of Gastroesophageal Reflux in Infants and Children





