Two peer-reviewed studies. One says 43% of pregnancies after a neuromyelitis optica diagnosis end in miscarriage. The other says 8%.
Table of Contents
Both are correct. They are describing different women.
That single fact explains why most articles on neuromyelitis optica and pregnancy leave readers more frightened than informed. The number that applies to you depends almost entirely on one variable, and it is a variable you can change.
| Quick Answer Pregnancy with neuromyelitis optica spectrum disorder (NMOSD) raises the risk of miscarriage and preeclampsia above general population rates. Unlike multiple sclerosis, NMOSD does not go quiet during pregnancy. The sharpest danger window is the first three months after delivery, when relapse rates climb three to eight times above baseline. With controlled disease and a planned care team, most women deliver healthy babies. |
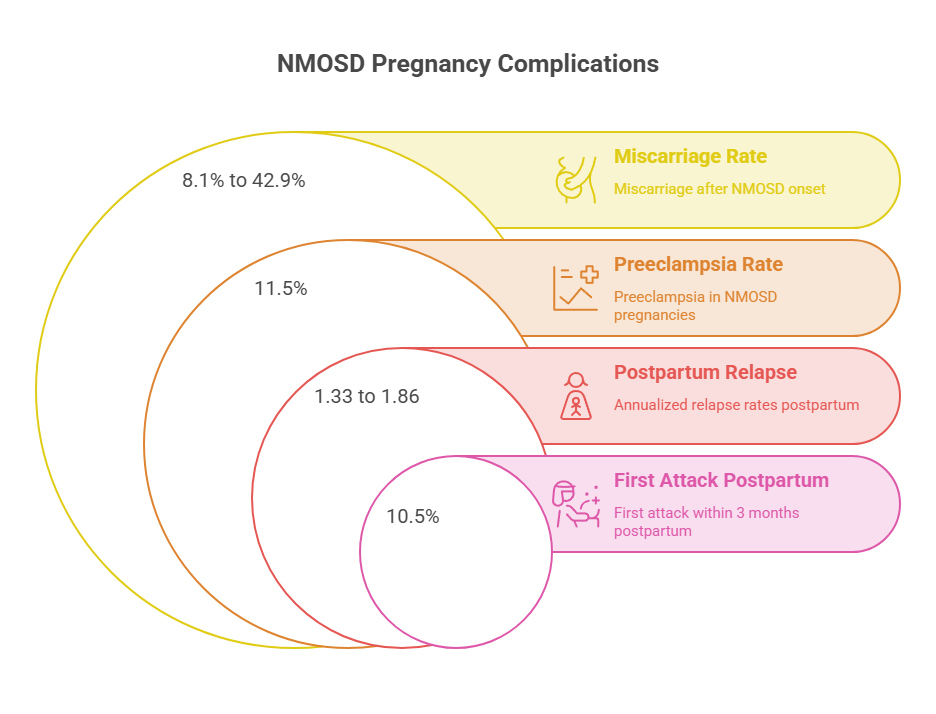
| At a Glance Reported miscarriage rates after NMOSD onset range from 8.1% to 42.9%; disease activity at conception explains nearly all of that gapPreeclampsia affects roughly 11.5% of NMOSD pregnancies versus about 3% of pregnancies overallNMOSD disease activity does not fall during pregnancy the way multiple sclerosis doesRelapse risk peaks in the first 3 months postpartum, with annualized relapse rates of 1.33 to 1.86About 10.5% of women whose NMOSD began before age 40 had their first-ever attack within 3 months of giving birthFertility appears mildly impaired, and roughly 6% of women with NMOSD needed fertility treatment to conceiveStopping immunosuppressive therapy in order to conceive is the most common preventable mistake in this populationRituximab and azathioprine carry the most pregnancy data; the four newer FDA-approved NMOSD drugs carry the least |
Why Neuromyelitis Optica and Pregnancy Collide So Often
NMOSD is not a disease that occasionally happens to affect pregnant women. It lands, with statistical precision, on women during the exact years they are building families.
The US Picture: Who Actually Has NMOSD
An analysis of electronic health records covering 25.7 million Americans estimated roughly 21,600 people living with NMOSD in the United States, about 15,400 of them women. That puts prevalence somewhere near 7 to 9 per 100,000.
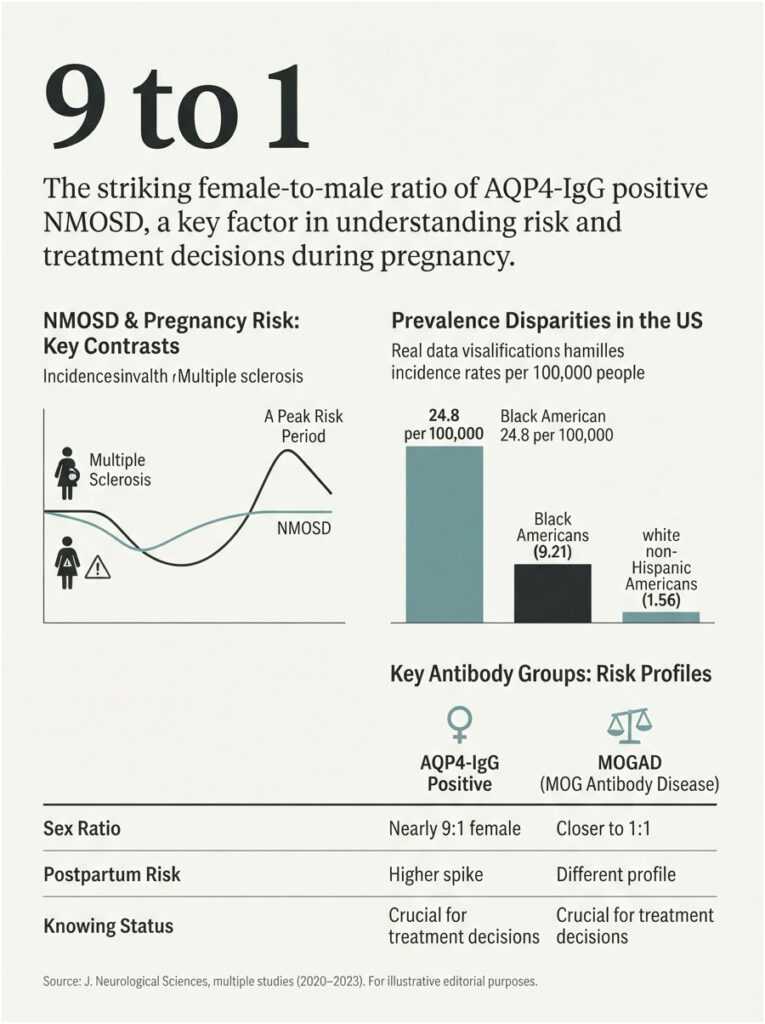
The burden is not evenly distributed. A Kaiser Permanente Southern California cohort tracking new diagnoses from 2010 to 2021 found the age- and sex-standardized incidence in Black Americans was 9.21 per million person-years, compared with 1.56 in white non-Hispanic Americans.
Asian American and Hispanic American women also carry disproportionate risk. Prevalence estimates for Black American women reach 24.8 per 100,000, the highest of any US demographic group.
Why the Timing Overlaps With Childbearing Years
Aquaporin-4 antibody positive NMOSD, which accounts for over 75% of cases, has a female-to-male ratio approaching 9 to 1. Median onset falls between the early 30s and early 40s depending on which cohort you read.
Put those two numbers together and the overlap is structural. A large share of women receive this diagnosis in the middle of their reproductive planning.
Patients who come to HealthCareOnTime after an AQP4-IgG positive result almost always ask the same question within the first minute: can I still have children? The honest answer is yes, with conditions attached.
NMOSD Is Not Multiple Sclerosis, and That Changes Everything
This is the most consequential paragraph in this article. Multiple sclerosis famously goes quiet during pregnancy, with relapse rates dropping sharply in the second and third trimesters. Many women absorb that reassurance and assume it applies to them.
It does not. In NMOSD, disease activity does not subside during pregnancy, and in some cohorts it rises. Every piece of MS pregnancy advice a newly diagnosed woman has read online may be the wrong advice for her.
Our medical reviewers see this confusion constantly. A woman is told her autoimmune neurological condition will improve during pregnancy, stops her medication, and relapses at 17 weeks.
Not All NMOSD Behaves the Same Way
Your antibody status matters more than your diagnosis label, and almost no article on this topic says so.
AQP4-IgG positive NMOSD is the disease this article is mostly describing. It carries the 9-to-1 female predominance, the placental antibody mechanism, and the postpartum relapse spike. The pregnancy data is overwhelmingly drawn from these women.
Seronegative NMOSD is less understood. Relapse risk during and after pregnancy appears lower than in AQP4-positive disease, though the studies are small and most enrolled only a minority of seronegative patients.
MOG antibody disease (MOGAD) was once folded into NMOSD and is now recognized as a separate condition. Its sex ratio sits closer to 1 to 1, and its pregnancy behavior differs. In one French multicenter cohort, the postpartum relapse spike was concentrated among AQP4-positive women, not MOG-positive ones.
If you do not know your antibody status, that test comes before every other decision on this page. It changes the risk numbers you are actually looking at.
Before You Conceive: Fertility, Timing, and the Twelve-Month Rule
Most pages about NMOSD and pregnancy start at conception. The decisions that matter most are made twelve months earlier.
Does NMOSD Affect Fertility?
Probably, mildly. Fecundity in NMOSD is likely impaired, and animal studies point toward reduced fertility rates. Human data is thin.
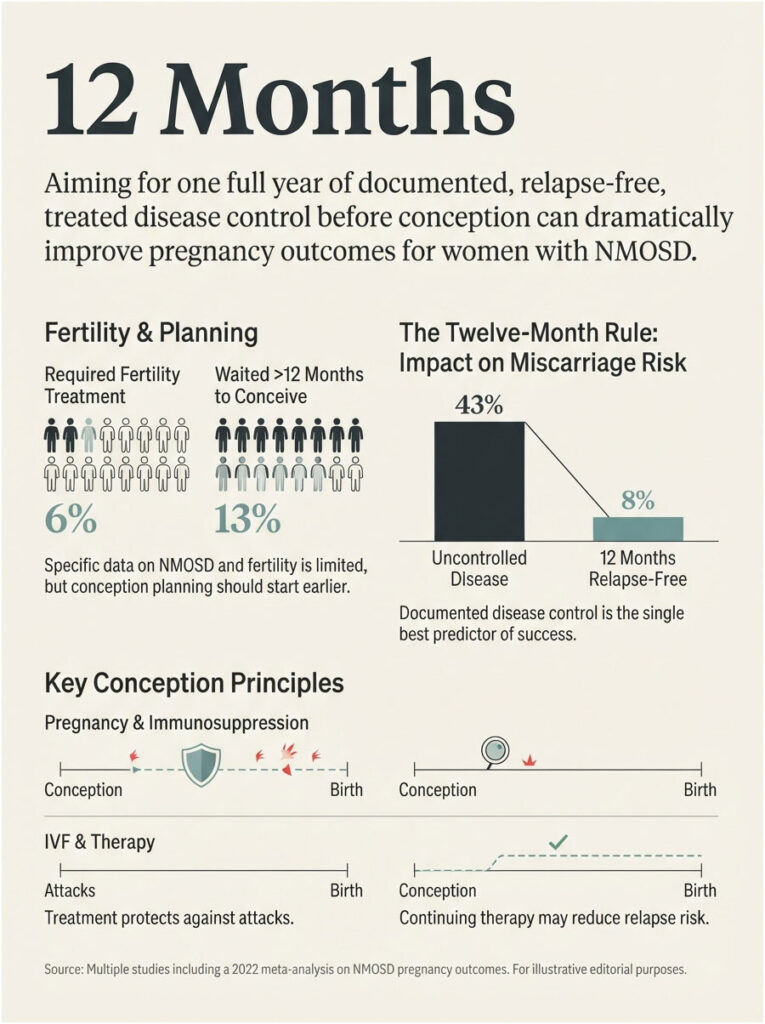
What exists is worth knowing. In studied populations, roughly 6% of women with NMOSD required fertility treatment, and about 13% waited more than twelve months to conceive.
Neither figure is catastrophic. Both are higher than background, and both argue for starting your planning conversation earlier than you otherwise would.
The Twelve-Month Rule
The single strongest predictor of a good NMOSD pregnancy is disease control before conception. Not during. Before.
The 2022 meta-analysis of fifteen studies found that immunosuppressive treatment during pregnancy and older age at conception were both associated with protection against pregnancy-related attacks. Treatment was protective, not harmful.
The practical translation most neuroimmunologists give: aim for twelve months of documented, relapse-free, treated disease before you try to conceive. That window is what separates the 8% miscarriage rate from the 43% one.
IVF and Assisted Reproduction: An Honest Data Gap
Here is something no other page will tell you plainly. There is essentially no NMOSD-specific data on in vitro fertilization.
What exists comes from multiple sclerosis, where a 2025 study found that maintaining disease-modifying therapy until IVF was the determining factor in reducing relapse risk. Ovarian stimulation with GnRH analogs can provoke disease activity in autoimmune neurological conditions.
Whether that transfers to NMOSD is unknown. Given that NMOSD relapses recover far worse than MS relapses, the conservative reading is to treat ovarian stimulation as a period of elevated risk and to stay on therapy through it. That is a conversation for a neuroimmunologist and a reproductive endocrinologist together, not either one alone.
What Research Actually Says About Complication Risks
Here is where the numbers get contradictory, and where careful reading pays off.
Miscarriage, and Why Two Studies Disagree So Loudly
The 42.9 Percent Figure
In 2015, an international team led from the University of Oxford published a retrospective cohort in Neurology covering 60 women with AQP4-positive NMOSD across the UK, Portugal, and Japan, spanning 126 pregnancies.
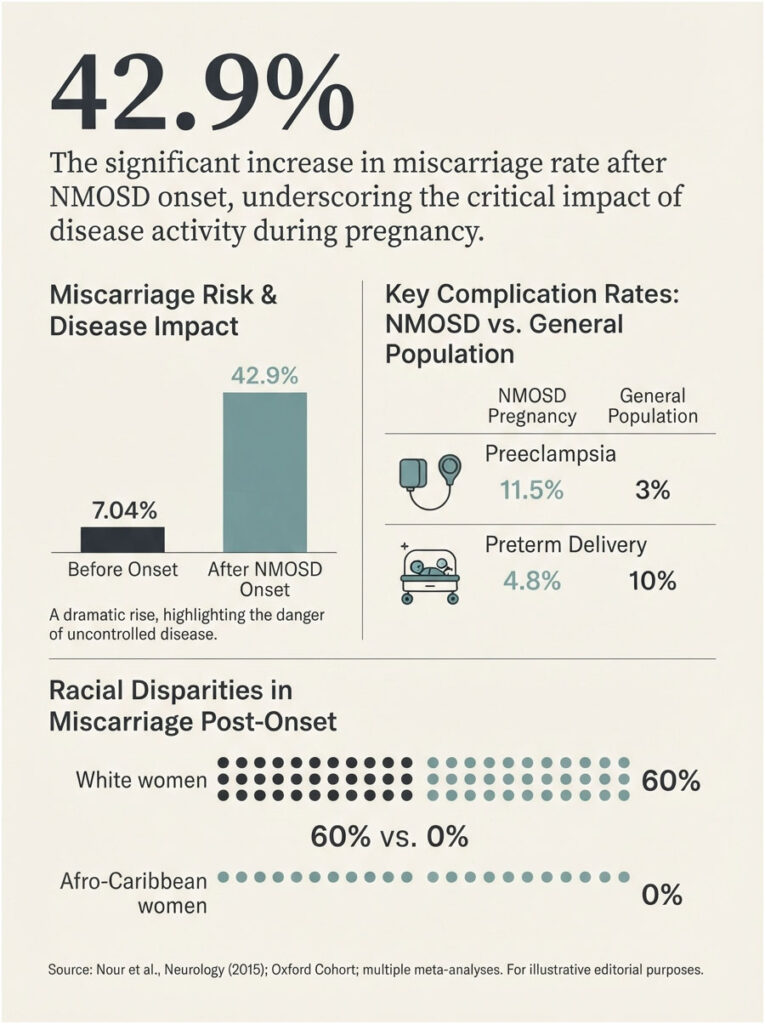
Their finding: the miscarriage rate in pregnancies occurring after NMOSD onset was 42.9%, against 7.04% in pregnancies before onset. The odds ratio for miscarriage after onset was 7.28.
The number that made every headline was 43%. What got lost was the mechanism. Miscarriages clustered in women with high disease activity, not in women taking medication. The annualized relapse rate in pregnancies ending in miscarriage was roughly 0.71, far above that of viable pregnancies.
There was also a striking racial split. Among white women in that cohort, the post-onset miscarriage rate was 60%. Among Afro-Caribbean women, it was zero.
The 8.1 Percent Figure
A later meta-analysis pooled fifteen studies covering 443 women with NMOSD and 639 pregnancies. It reported 8.1% spontaneous abortions, 2.7% preeclampsia, 4.8% premature deliveries, and 5.3% neonatal complications.
Those figures are dramatically lower. They also come from a larger, more recent, and considerably better-treated population.
What the Gap Actually Tells You
The variable separating a 43% miscarriage rate from an 8% one is not luck, not race, and not maternal age. It is disease activity at conception.
Women who conceive during or near an active disease period miscarry at alarming rates. Women who conceive after twelve months of controlled, treated, relapse-free disease do not.
That reframing changes what you do with the rest of this article. The risk is not fixed. It is a function of timing and treatment, and both are in your control.
Preeclampsia: Roughly Triple the Background Rate
The same Oxford cohort reported a preeclampsia rate of 11.5% (95% CI 6.27% to 18.9%) across 113 pregnancies in 57 women. Background rates in the general population run near 3%.
The odds climbed further in women carrying a second autoimmune diagnosis or who had miscarried in their most recent prior pregnancy. NMOSD onset timing itself was not an independent predictor, which points toward a broader autoimmune driver rather than NMOSD acting alone.
Across the autoimmune antibody panels processed through our diagnostic network, women who carry AQP4-IgG frequently carry a second autoantibody as well. That overlap is exactly what pushes preeclampsia odds upward, and it is exactly what a preconception screen catches.
Preterm Birth, Growth Restriction, and Stillbirth
Pooled data puts premature delivery at 4.8%, actually below the roughly 10% national preterm rate reported by the CDC. That is genuinely reassuring and deserves to be said plainly.
Less reassuring: a 2025 single-center cohort found six of nine pregnancies experienced adverse outcomes, including premature rupture of membranes, intrauterine growth restriction, preterm birth, postpartum hemorrhage, stillbirth, and low birth weight.
The case literature is also honest about the worst case. One documented US case involved a woman with seropositive NMO who discontinued all medication in the first trimester, relapsed repeatedly, and presented at 31 weeks with eclampsia, HELLP syndrome, and fetal death.
That outcome is not the norm. It is what an uncontrolled NMOSD pregnancy can look like at its worst, and it is why preconception planning gets treated as urgent rather than optional.
| Complication | Rate in NMOSD | Rate in General US Pregnancy | Signal Strength | Source |
| Miscarriage (pregnancies after NMOSD onset) | 42.9% | 10% to 15% | Strong, but activity-dependent | Nour et al., Neurology, 2015 |
| Spontaneous abortion (pooled, treated population) | 8.1% | 10% to 15% | Neutral when disease is controlled | Meta-analysis, 443 patients / 639 pregnancies |
| Preeclampsia | 11.5% | About 3.1% | Strong | Nour et al., Neurology, 2015 |
| Preterm delivery | 4.8% | About 10.4% (CDC) | Neutral to favorable | Meta-analysis, 443 patients |
| Neonatal complications | 5.3% | Varies by definition | Modest | Meta-analysis, 443 patients |
| Relapse, first 3 months postpartum (ARR) | 1.33 to 1.86 | Not applicable | Very strong | Neurology 2017; JAMA Neurology 2022 |
The Postpartum Window: The Biggest Risk You Can Plan For
If you take one section of this article to your neurologist, take this one.
The relapse data is unusually consistent across countries, cohorts, and decades. Disease activity climbs modestly during pregnancy, dips slightly in the third trimester, then detonates in the first twelve weeks after delivery.
| Pregnancy Phase | Annualized Relapse Rate | What This Means Clinically | Source |
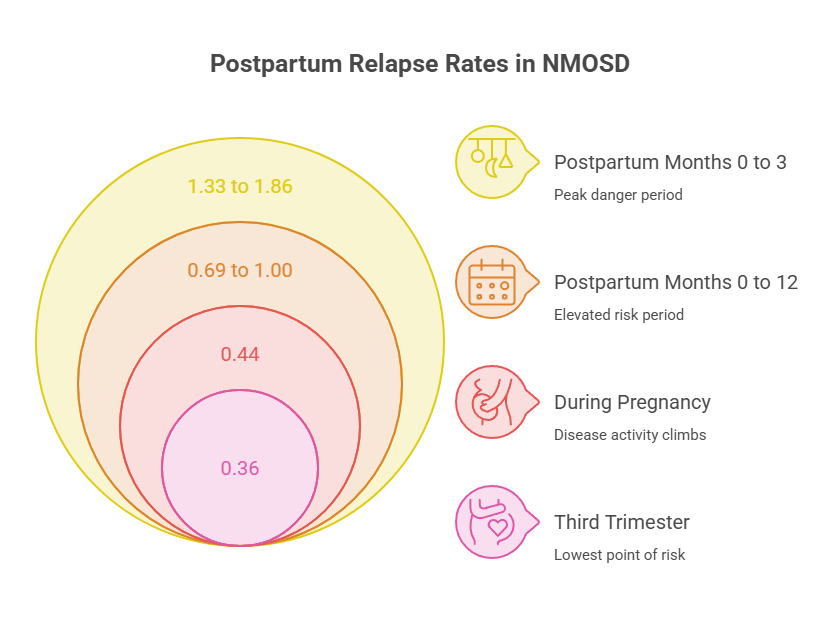
| 2 years pre-pregnancy (baseline) | 0.17 | Reference point | Kim et al., Neurology, 2017 (217 US women, 7 centers) |
| During pregnancy, all trimesters | 0.44 | Risk rises; it does not fall | Kim et al., Neurology, 2017 |
| Third trimester | 0.36 | Lowest point of the entire cycle | JAMA Neurology meta-analysis, 2022 |
| Postpartum months 0 to 3 | 1.33 to 1.86 | Peak danger window | Neurology 2017; JAMA Neurology 2022 |
| Postpartum months 0 to 12 | 0.69 to 1.00 | Elevated for a full year | Neurology 2017; Scientific Reports 2025 |
| Chinese cohort, 202 pregnancies, first postpartum trimester | 1.44 (vs 0.23 pre-pregnancy) | Pattern replicates across populations | Reported in Autoimmunity Reviews, 2023 |
The 2022 meta-analysis of fifteen studies found the highest annualized relapse rate at 1.86 (95% CI 1.47 to 2.25) in postpartum months zero to three. The lowest, 0.36, fell in the third trimester.
A 2025 cohort reported that 76.9% of all observed relapses occurred postpartum. Not most. Roughly three out of four.
Why NMOSD Behaves the Opposite of MS
The working explanation involves the immune shift pregnancy produces. Rising estrogen creates a pro-inflammatory environment in NMOSD rather than a protective one, and the ratio of Th17 cells to regulatory T cells climbs.
Whatever the precise mechanism, the clinical consequence is settled. Do not expect a pregnancy honeymoon. Plan for a postpartum storm.
When NMOSD Starts After Delivery
Here is a fact that catches even neurologists off guard. Among women whose NMOSD began before age 40, 10.5% experienced their first-ever attack during the three months after childbirth, a rate 2.9 times higher than chance would predict.
The postpartum period is not only a relapse window for women who already have NMOSD. It is a common debut window for women who do not yet know they have it.
Patients commonly ask us why a new mother with sudden vision loss or leg weakness gets told she is simply exhausted. That misattribution costs vision and mobility, and a single antibody test prevents it.
The Disability Cost of a Postpartum Relapse
NMOSD attacks recover badly. That is the defining difference between this disease and multiple sclerosis, and it is why the postpartum window carries so much weight.
Pooled data shows Expanded Disability Status Scale scores worsening by a mean of 0.44 points during pregnancy and 0.88 points postpartum. One cohort tracked EDSS climbing from 1.56 before pregnancy to 2.1 at six months after delivery.
Those are not temporary dips. In NMOSD, disability accumulates attack by attack, and what you lose in a postpartum relapse you may not get back.
The Biology: How AQP4 Antibodies Reach the Placenta
Understanding the mechanism makes the risk numbers stop feeling arbitrary.
Aquaporin-4 Sits in Placental Tissue, Not Just the Brain
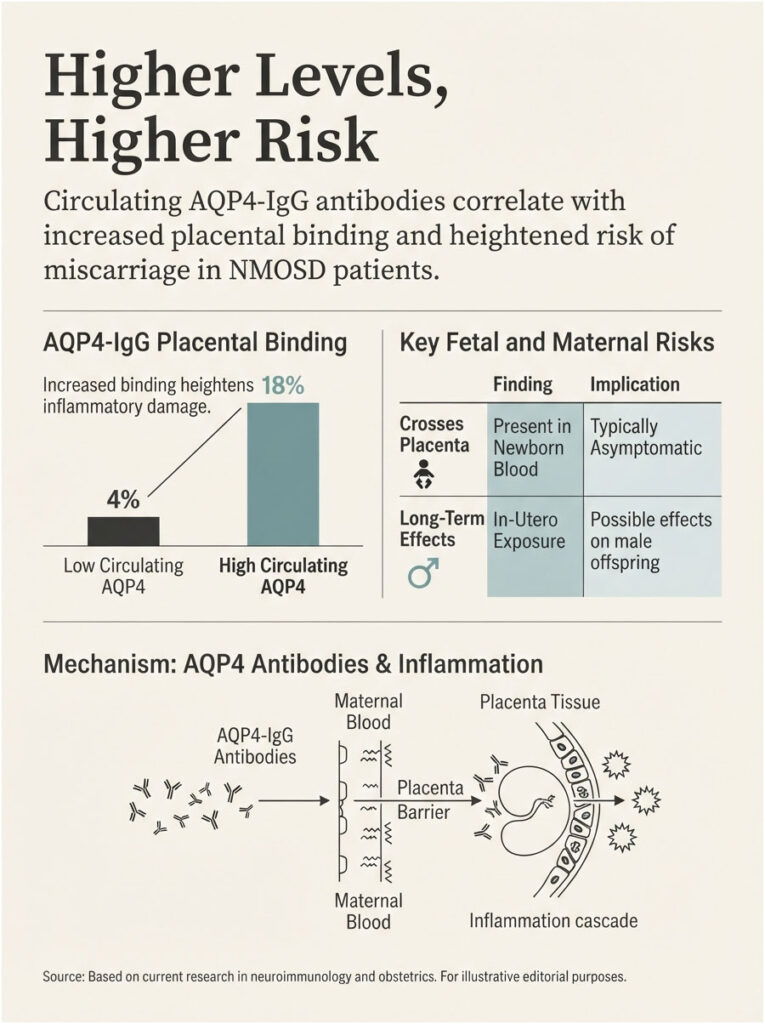
Aquaporin-4 is the water channel protein that AQP4-IgG antibodies attack in the optic nerve and spinal cord. It is also expressed at high levels in the placenta.
When AQP4-IgG binds placental tissue, it can trigger complement activation and inflammatory damage in the same way it damages astrocytes in the central nervous system. That is the bridge between an eye-and-spine disease and a first-trimester miscarriage.
It also explains why disease activity matters so much. Higher circulating antibody levels mean more placental binding.
What Crosses to the Baby
AQP4 antibodies do cross the placenta and can be measured in newborn blood. In most cases they cause no symptoms, and the infant clears them over the following months.
Research from the Feinstein Institutes for Medical Research, published in Science Translational Medicine, found that in-utero exposure to AQP4 antibodies during a critical developmental window produced long-term effects in offspring, with male offspring disproportionately affected.
That work was done in animal models. The human significance is unknown, and the researchers said so directly. Follow-up studies of children born to mothers with NMOSD are now underway.
The PRES and Eclampsia Overlap
Because aquaporin-4 governs bidirectional water movement in the brain, some researchers have proposed that AQP4 antibodies may contribute to posterior reversible encephalopathy syndrome (PRES).
PRES appears in NMOSD patients without eclampsia, and it appears commonly in eclampsia. The overlap may be additive rather than coincidental, which is one more argument for treating blood pressure monitoring as non-negotiable.
Medication Decisions Before, During, and After Pregnancy
This is the section most women arrive looking for, and the one that current search results serve worst.
Drugs That Must Stop Before Conception
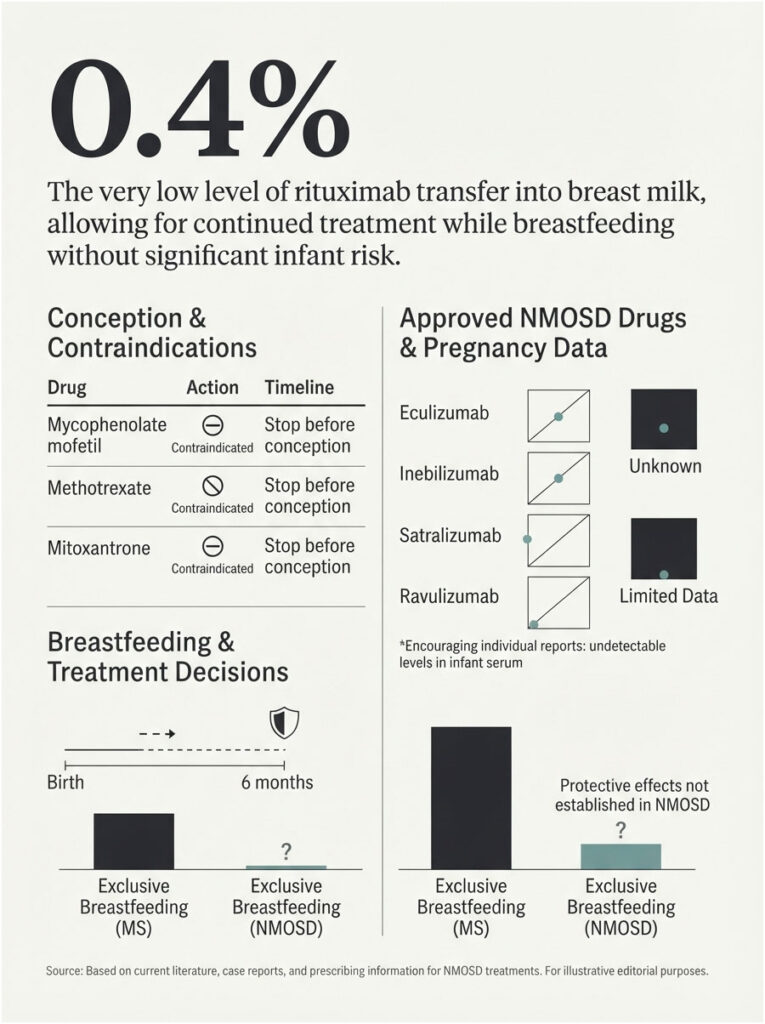
Mycophenolate mofetil (CellCept), methotrexate, and mitoxantrone are contraindicated in pregnancy. These are established teratogens and there is no gray area.
If you are taking any of them and want children, the conversation with your neurologist starts now, not later. Switching agents and completing a washout takes months, not weeks.
Drugs Most Often Continued
Azathioprine (Imuran) carries the most established pregnancy safety record among NMOSD immunosuppressants and is generally considered acceptable to continue through pregnancy and lactation.
Rituximab (Rituxan) is used off-label for NMOSD across the US and is widely continued or strategically timed around conception. The Cleveland Clinic’s published position is that rituximab may still be the preferred treatment when indicated, given the depth of experience with it relative to the newer agents.
The Four FDA-Approved NMOSD Drugs
Four targeted therapies are now FDA approved for AQP4-positive NMOSD: eculizumab (Soliris), inebilizumab (Uplizna), satralizumab (Enspryng), and ravulizumab (Ultomiris).
All four have limited pregnancy data. Limited data is not evidence of harm, and it is not evidence of safety. It is exactly what it sounds like.
Individual reports have been encouraging. In documented satralizumab pregnancies, the drug was undetectable in umbilical cord blood, infant serum, and breast milk. The Cleveland Clinic notes satralizumab may be a reasonable consideration based on prescribing information and the limited studies available.
Two active pregnancy registries are enrolling US patients right now: the ENSPRYNG Pregnancy Registry and the UPLIZNA pregnancy safety study. If you become pregnant on either drug, enrolling costs nothing and builds the evidence base the next woman will need.
| Drug (Brand) | Pregnancy Data Status | Common US Practice | Breastfeeding Signal |
| Azathioprine (Imuran) | Most established of any NMOSD agent | Frequently continued through pregnancy | Generally considered compatible |
| Rituximab (Rituxan) | Substantial off-label experience | Timed infusions or continued dosing | Relative infant dose under 0.4% |
| Satralizumab (Enspryng) | Limited; registry open | Case-by-case decision | Undetectable in milk in reported cases |
| Inebilizumab (Uplizna) | Very limited; registry open (NCT05909761) | Case-by-case decision | Unknown |
| Eculizumab (Soliris) | Limited; long safety record in other diseases | Case-by-case decision | Limited data |
| Mycophenolate (CellCept) | Known teratogen | Must be stopped before conception | Contraindicated |
| Methotrexate | Known teratogen | Must be stopped before conception | Contraindicated |
| IV methylprednisolone | Extensive | First-line for acute relapse in pregnancy | Timing-dependent, usually workable |
A pooled analysis presented at the American Academy of Neurology reported full-term birth rates of 67.6% with rituximab, 63.1% with tocilizumab, and 80.7% with eculizumab. Birth defects were infrequent across all three: 2.2%, 1.9%, and 0.1% respectively.
Treating an Acute Relapse While Pregnant
If you relapse while pregnant, you treat it. Intravenous methylprednisolone, plasma exchange, and intravenous immunoglobulin are all usable during pregnancy.
An untreated NMOSD attack is more dangerous to both mother and fetus than the treatment is. Permanent vision loss and paralysis are the alternatives sitting on the table.
Our medical team’s read of the current evidence is unambiguous here: hesitation is the risk, not the steroids.
Breastfeeding and Restarting Therapy
Rituximab transfers into breast milk at a relative infant dose below 0.4%, far under the 10% threshold generally treated as acceptable. Its poor oral bioavailability further limits any absorption by the infant.
That finding matters because too many women are told they must choose between treating their disease and feeding their baby. For rituximab, that choice is often a false one.
One caution worth repeating. Exclusive breastfeeding is protective against relapse in multiple sclerosis. That protection has never been demonstrated in NMOSD, and assuming it exists is a mistake with real consequences.
Building Your Care Team and Monitoring Plan
Who Belongs on the Team
A neuroimmunologist or an MS-and-NMOSD specialist neurologist, not a general neurologist. A maternal-fetal medicine (MFM) specialist, identified before conception rather than after a complication.
Add an obstetrician who has actually read your neurology notes, an ophthalmologist for baseline optic nerve documentation, and a laboratory that runs AQP4-IgG titers reliably and consistently.
What to Monitor and When
Blood pressure and urine protein at every prenatal visit, without exception. Serial growth ultrasounds beyond the standard schedule.
A documented baseline EDSS score before conception, so that postpartum change is measurable rather than guessed at. Baseline visual acuity, plus optical coherence tomography where available.
Women planning pregnancy who book antibody panels through HealthCareOnTime are often surprised to find a second autoantibody present. Given that a second autoimmune diagnosis raises preeclampsia odds, screening broadly before conception is worth the appointment.
Delivery Planning
Vaginal delivery is not contraindicated by NMOSD. Cesarean rates run higher in this population, but the driver is usually disability level and standard obstetric factors rather than the antibody itself.
Epidural anesthesia is generally acceptable. If you have a history of transverse myelitis, a documented pre-anesthesia neurological exam protects both you and your anesthesiologist.
| If This Is Your Situation | Then Do This | Who to Involve |
| Newly diagnosed, want children within 2 years | Delay conception until you have 12 months of documented relapse-free control | Neuroimmunologist |
| Currently taking mycophenolate or methotrexate | Switch agents and complete the full washout before trying | Neuroimmunologist plus MFM |
| On rituximab and planning pregnancy | Discuss timing infusions so conception falls inside the coverage window | Neuroimmunologist |
| Considering IVF | Stay on therapy through ovarian stimulation; treat it as a high-risk window | Neuroimmunologist plus reproductive endocrinologist |
| Pregnant and experiencing a new attack | Treat it now with IV steroids or plasma exchange; do not wait it out | Neurologist plus MFM, urgently |
| 36 weeks pregnant, disease stable | Confirm your postpartum therapy restart date before you deliver | Neurologist plus OB |
| Just delivered and want to breastfeed | Get drug-specific milk transfer data before deciding either way | Neurologist plus lactation consultant |
| First-ever vision loss or limb weakness after childbirth | Emergency evaluation; specifically request AQP4-IgG antibody testing | Emergency department plus neurologist |
Pitfalls That Cost Women Good Outcomes
Stopping Treatment Cold Turkey to Conceive
This is the most documented preventable error in NMOSD pregnancy. It feels like the responsible choice. It is not.
The Oxford cohort’s miscarriages clustered in women with high disease activity, not in women taking immunosuppressants. The 2022 meta-analysis found that immunosuppressive treatment during pregnancy was associated with reduced attack risk, not with increased complications.
Missing the Postpartum Restart Window
An international registry tracking pregnancies from 2020 through 2024 found that women with NMOSD resumed rituximab a median of 271 days after pregnancy completion. Not one restarted within the first three months.
The peak relapse window closes at 90 days. Restarting at 271 days means the entire high-risk period passed unprotected.
Calling Neurological Symptoms Normal Pregnancy
Numbness, bladder changes, visual disturbance, and unsteady gait all get written off as pregnancy or postpartum exhaustion. In NMOSD, these are attack signals until proven otherwise.
Assuming MS Advice Applies
Say it one final time, because it costs women their vision. Pregnancy protects against MS relapses. Pregnancy does not protect against NMOSD relapses.
Your Preconception to Postpartum Action Plan
- Twelve or more months before conception. Achieve documented, relapse-free disease control. Move off any teratogenic agent. Confirm your antibody status.
- Six months before. Complete the washout period. Establish baseline EDSS, AQP4-IgG titer, visual acuity, and a full autoimmune antibody screen.
- Three months before. Assemble the team. Identify your maternal-fetal medicine specialist while you are still not pregnant.
- First and second trimesters. Continue the agreed therapy. Blood pressure and urine protein at every visit. Serial growth ultrasounds.
- Third trimester. Relapse risk is at its lowest point of the entire cycle here. Use that calm to write the postpartum plan down, on paper, with dates on it.
- Delivery. Neurological baseline documented before any anesthesia is administered.
- Days 0 through 90 postpartum. The high-alert window. Therapy restarts on the pre-written schedule. Your threshold for calling the neurologist should be uncomfortably low.
- Months 3 through 12. Risk stays elevated for a full year. Do not relax monitoring at the three-month mark.
Return, for a moment, to the two numbers this article opened with. Forty-three percent and eight percent, both true, both published, both describing women with the same diagnosis.
Which number describes you is not decided by fate. It is decided in the twelve months before you conceive.
Frequently Asked Questions
Can you have a healthy baby with neuromyelitis optica?
Yes. Most women with well-controlled NMOSD deliver healthy babies. Pooled data across 639 pregnancies shows preterm delivery at 4.8% and neonatal complications at 5.3%, both close to or below general population figures. Outcomes track with disease activity at conception rather than with the diagnosis itself.
Does neuromyelitis optica cause miscarriage?
It raises the risk, particularly when disease is active. AQP4 antibodies bind aquaporin-4 in placental tissue and can trigger inflammatory damage there. Women who conceive during periods of high disease activity miscarry at far higher rates than women who conceive after twelve months of controlled, treated disease.
What is the actual miscarriage rate with NMOSD?
Published figures range from 8.1% to 42.9%. The 42.9% figure comes from a 2015 cohort where miscarriages clustered in women with high relapse activity. The 8.1% figure comes from a larger, better-treated pooled population. Disease control at conception is what separates those two numbers.
Does pregnancy make neuromyelitis optica worse?
Often, yes. Unlike multiple sclerosis, NMOSD does not remit during pregnancy. Annualized relapse rates rise from roughly 0.17 at baseline to 0.44 during pregnancy. Disability scores worsen by a mean of 0.44 EDSS points across pregnancy and 0.88 points in the postpartum period.
When is relapse risk highest, during pregnancy or after?
After. The first three months postpartum carry annualized relapse rates of 1.33 to 1.86, roughly eight to eleven times the pre-pregnancy baseline of 0.17. One cohort found nearly 77% of all relapses occurred postpartum. Risk stays elevated for a full twelve months.
Do AQP4 antibodies cross the placenta to my baby?
Yes. AQP4-IgG antibodies cross the placenta and are measurable in newborn blood. In most cases they cause no symptoms, and the infant clears them over subsequent months. Animal research suggests possible long-term neurodevelopmental effects from in-utero exposure, but human significance remains unknown.
Is neuromyelitis optica hereditary?
NMOSD is not inherited in any straightforward genetic pattern. Your child will not be born with the disease. A general autoimmune predisposition can run in families, but the overwhelming majority of children born to mothers with NMOSD never develop it.
Does NMOSD affect fertility?
Mildly, based on limited data. Fecundity appears somewhat impaired, with roughly 6% of women requiring fertility treatment and about 13% waiting more than twelve months to conceive. Neither figure is alarming, but both argue for starting your preconception planning earlier than you might otherwise.
Is rituximab safe during pregnancy for NMOSD?
Rituximab carries the deepest off-label pregnancy experience of any NMOSD therapy, and the Cleveland Clinic notes it may still be preferred when treatment is indicated. Pooled data shows a full-term birth rate of 67.6% and a birth defect rate of 2.2%. Timing of infusions relative to conception matters considerably.
Can I take Uplizna or Enspryng while pregnant?
Pregnancy data for both is limited, which is not the same as evidence of harm. Satralizumab (Enspryng) was undetectable in cord blood and breast milk in reported cases. Active pregnancy registries are enrolling patients on both drugs, and enrollment is free and worth considering.
Can I breastfeed with neuromyelitis optica?
Frequently, yes. Rituximab appears in breast milk at a relative infant dose below 0.4%, far under the 10% threshold generally considered acceptable. Get drug-specific data before deciding. Note also that the breastfeeding relapse protection seen in multiple sclerosis has not been demonstrated in NMOSD.
Can NMOSD be diagnosed for the first time after childbirth?
Yes, and this is badly underrecognized. Among women with NMOSD onset before age 40, 10.5% had their first attack within three months of delivering, a rate 2.9 times higher than expected. New vision loss, limb weakness, or bladder dysfunction after childbirth warrants AQP4-IgG testing, not reassurance.
| Medical Disclaimer This content is educational and is not medical advice. NMOSD pregnancy management is highly individual and depends on your antibody status, disease history, current therapy, and obstetric picture. Do not start, stop, or change any medication without your neurologist. New vision loss, limb weakness, or bladder dysfunction requires immediate medical evaluation. |
References
- Pregnancy outcomes in aquaporin-4-positive neuromyelitis optica spectrum disorder, Neurology (Nour et al., 2015)
- High risk of postpartum relapses in neuromyelitis optica spectrum disorder, Neurology (Kim et al., 2017)
- Analysis of pregnancy-related attacks in NMOSD: systematic review and meta-analysis, JAMA Neurology (2022)
- Risks and outcomes of pregnancy in neuromyelitis optica spectrum disorder, Autoimmunity Reviews (2023)
- Neuromyelitis optica spectrum disorders and pregnancy: therapeutic considerations, Nature Reviews Neurology (2020)
- Insights into NMOSD and pregnancy: single-center cohort, Scientific Reports (2025)
- The epidemiology and clinical presentation of seropositive NMOSD in a US population, Annals of Clinical and Translational Neurology (2025)
- Racial and ethnic disparities in the incidence of NMOSD, Neurology (Kaiser Permanente Southern California)
- Women’s Health in Neuromyelitis Optica Spectrum Disorder, Cleveland Clinic
- Minimal breast milk transfer of rituximab, Neurology: Neuroimmunology and Neuroinflammation
- Pregnancy outcomes in NMOSD: meta-analysis of pharmacotherapeutic agents, Neurology (AAN abstract)
- Assessing the risk of relapse after in vitro fertilization, Neurology: Neuroimmunology and Neuroinflammation (2025)
- NMOSD relapse rates by serostatus and postpartum trimester, NeurologyLive
- In-utero AQP4 antibody exposure research, Feinstein Institutes for Medical Research
- Satralizumab during pregnancy and breastfeeding: case report, Frontiers in Neurology
- MSBase Pregnancy, Neonatal Outcomes and Women’s Health Registry (2020 to 2024), Multiple Sclerosis Journal
- Neuromyelitis optica in pregnancy complicated by PRES, eclampsia and fetal death (case report)
- UPLIZNA (inebilizumab) pregnancy safety study, ClinicalTrials.gov NCT05909761
- ENSPRYNG (satralizumab) Pregnancy Registry