
You feel the symptoms. Muscle cramps that wake you at 2 a.m., a flutter in your chest, fatigue that coffee can’t touch, and sleep that never feels deep. Your doctor orders a magnesium test, the result comes back “normal,” and you’re sent home with a shrug. Here’s the part nobody mentioned: the standard test reads roughly 1% of the magnesium in your body.
Table of Contents
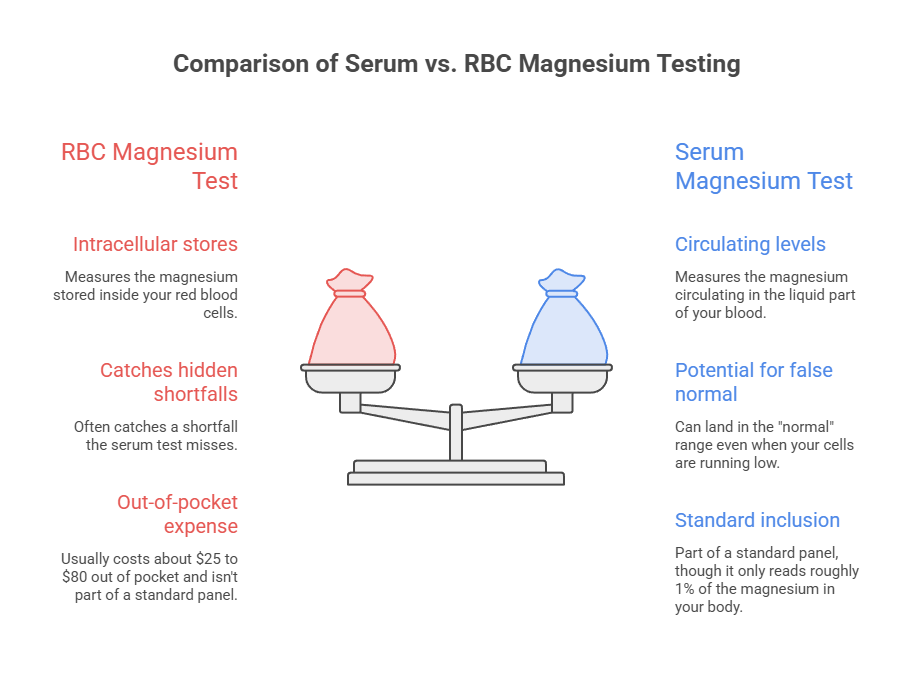
Quick answer: An RBC magnesium test measures the magnesium stored inside your red blood cells, while a serum magnesium test measures the magnesium circulating in the liquid part of your blood. Because only about 1% of the body’s magnesium sits in serum, a serum result can land in the “normal” range even when your cells are running low. The RBC test reflects intracellular stores, so it often catches a shortfall the serum test misses.
At a Glance
- Serum measures circulating magnesium (about 1% of body stores); RBC measures magnesium inside your cells.
- Red blood cell magnesium runs roughly three times higher in concentration than serum.
- Serum can sit squarely in the normal range during a genuine deficiency.
- A typical RBC magnesium range is about 4.0 to 6.8 mg/dL, depending on the lab.
- The RBC test usually costs about $25 to $80 out of pocket and isn’t part of a standard panel.
- Best candidates include people on diuretics or acid-reducing drugs, those with type 2 diabetes or gut conditions, heavy drinkers, and older adults.
That gap between “your labs are fine” and “but you feel terrible” is exactly where the RBC magnesium test earns its place. Our medical reviewers see the confusion often, because the two tests sound interchangeable and aren’t. One looks at the magnesium passing through your bloodstream right now. The other looks at the magnesium your cells have actually banked.
This guide breaks down what each test measures, why a serum number can mislead you, what a normal RBC magnesium range looks like, the symptoms that should prompt testing, and when it’s worth asking for the red blood cell version. Everything below is sourced to US authorities like the National Institutes of Health and the Institute of Medicine, with a plain-English read on what the numbers mean for you.
What an RBC Magnesium Test Actually Measures
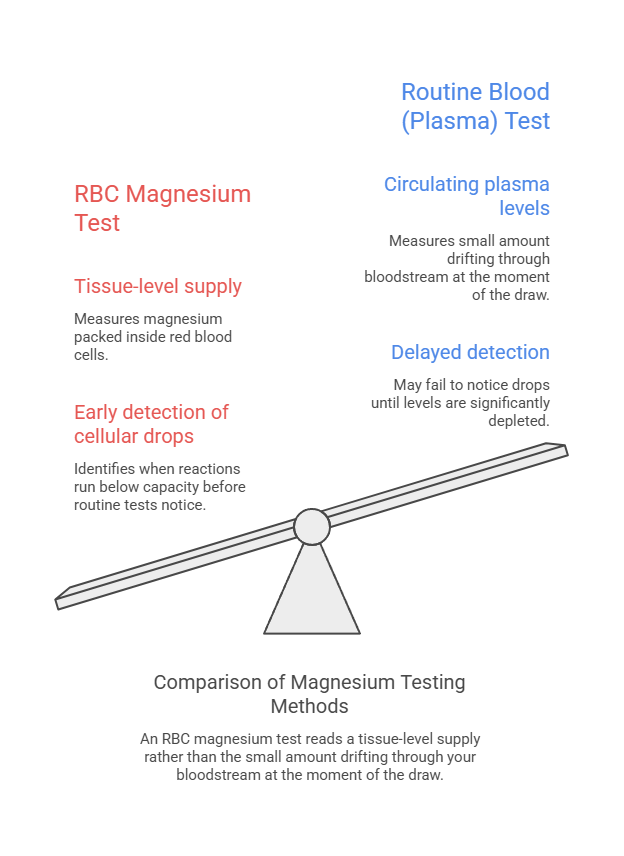
An RBC magnesium test (also called red blood cell magnesium or erythrocyte magnesium) measures how much magnesium is packed inside your red blood cells. Red cells store far more magnesium than the surrounding plasma does. So the test reads a tissue-level supply rather than the small amount drifting through your bloodstream at the moment of the draw.
That distinction matters because magnesium is a workhorse mineral. It acts as a cofactor in more than 300 enzyme reactions that handle energy production, muscle and nerve signaling, blood sugar control, and a steady heartbeat, according to the Institute of Medicine. When cellular magnesium drops, those reactions run below capacity long before a routine blood test notices.
Where magnesium lives in your body (the 1% vs 99% split)
The average adult body holds roughly 25 grams of magnesium. Most of it is locked away where a simple blood draw can’t see it: around 50 to 60% sits in bone, about 27% in muscle, and the rest in soft tissue, per Institute of Medicine reference data.
Only about 1% of your total magnesium floats in the blood outside your cells. That’s the slice a serum test samples. Picture a reservoir behind a dam; the serum test reads the water spilling over the top, not the volume held back in the basin.
Because the body works hard to keep that spillover steady, your serum number can look reassuring while the reservoir behind it quietly drains. The RBC test, by contrast, dips into the stored supply, which is why it tends to register a decline earlier.
How the lab runs the test (ICP-MS, specimen handling, CPT 83735)
Most US labs measure RBC magnesium using inductively coupled plasma mass spectrometry, a precise method for trace minerals, as LabCorp documents for its test. The billing code is CPT 83735, the same code used for magnesium testing generally.
The sample handling is fussier than a basic blood test. After the draw, the tube has to be spun so the plasma can be separated and discarded, leaving only the packed red cells, often within about two hours. That step is what lets the lab measure the magnesium inside the cells rather than around them.
Patients booking tests through HealthCareOnTime often ask why the timing is so strict. The short version: if the cells aren’t separated promptly, magnesium can shift between the plasma and the cells, and the result loses its meaning.
RBC Magnesium vs Serum Magnesium: The Core Difference
The serum magnesium test is the one you’ve almost certainly had. It’s quick, cheap, and bundled into many standard panels. It tells you whether the magnesium in your blood right now is dangerously high or low, which is useful in a hospital or an emergency.
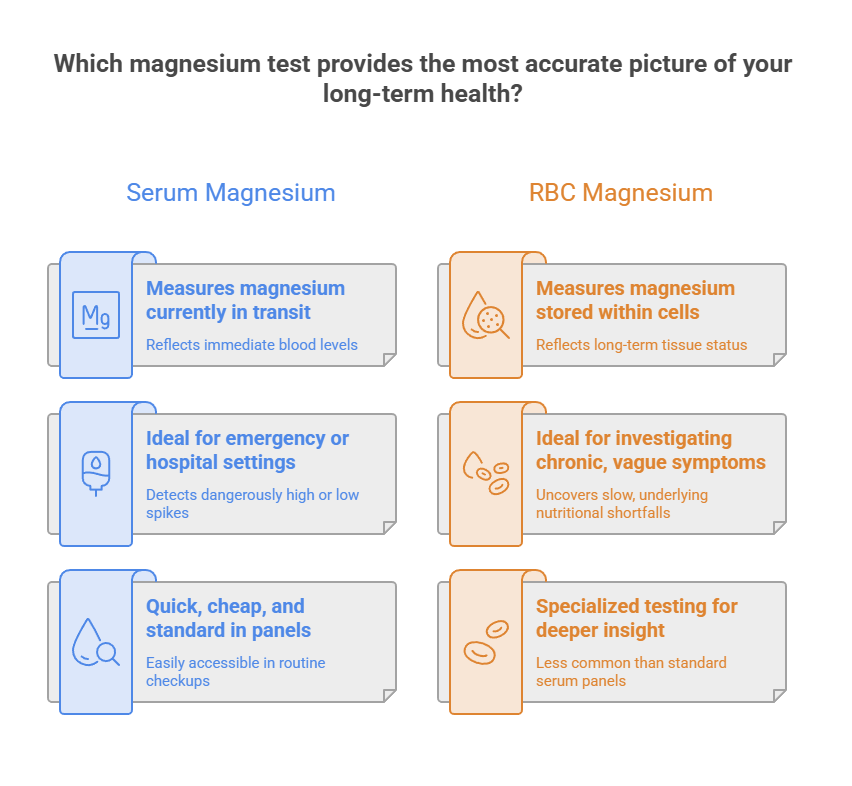
What it doesn’t do well is catch a slow, chronic shortfall. That’s the difference in one line: serum tracks the magnesium in transit; RBC tracks the magnesium in storage. For a person with vague, ongoing symptoms, the storage number usually tells the more honest story.
Why serum can read “normal” during a deficiency
Your body treats blood magnesium like a thermostat setting it refuses to let drift. When dietary intake falls short, it pulls magnesium out of cells and bone to top off the bloodstream. The serum level holds steady while the cellular and skeletal reserves shrink.
The kidneys reinforce this. They reabsorb more than 80% of the magnesium they filter when the body senses a shortage, clamping down on losses to defend the circulating level, as described in NHANES-based research. So a “normal” serum result can reflect a body that’s pulling from its own reserves to keep up appearances.
This is the trap behind the panic search. When readers contact HealthCareOnTime about a normal magnesium result that doesn’t match how they feel, the serum-versus-storage mechanism is usually the missing piece. Researchers from the NIH have even argued the serum reference range itself may be set too low, leaving people in a gray zone that gets labeled healthy, per a review on interpreting magnesium status.
What each test is genuinely good at
Neither test is “bad.” They answer different questions. The serum test is the right tool for acute swings and routine screening. The RBC test is the better tool for spotting a chronic, low-grade shortfall that hasn’t yet crashed your blood level.
The table below lays the two side by side so you can see where each one shines and where it falls short. The figures reflect typical US lab values; your own lab’s range will print on your report.
| Feature | Serum Magnesium Test | RBC Magnesium Test | Why It Matters |
| What it measures | Magnesium in blood plasma (circulating) | Magnesium inside red blood cells (stored) | Storage reflects long-term status; circulation reflects the moment |
| Share of body magnesium captured | About 1% | A tissue-level pool, roughly 3x serum concentration | A bigger window means fewer missed shortfalls |
| Sensitivity to early shortfall | Low; often normal until deficiency is severe | Higher; flags decline weeks to months sooner | Earlier detection means earlier correction |
| Typical normal range | About 1.8 to 2.3 mg/dL | About 4.0 to 6.8 mg/dL (lab-dependent) | RBC values run higher because cells hold more |
| Typical out-of-pocket cost | Often included in basic panels | About $25 to $80 | RBC is an add-on you usually request |
| Best use | Acute care, routine screening, kidney monitoring | Chronic symptoms, supplement tracking, at-risk groups | Match the test to the question |
Our medical team treats this comparison as the heart of the decision. If your only goal is a quick screen, serum does the job. If you’re chasing symptoms that a normal serum result hasn’t explained, the RBC test is the one worth asking about.
Signs Your Magnesium Might Be Running Low
Low magnesium rarely announces itself with one dramatic symptom. It shows up as a cluster of small complaints that are easy to blame on stress, age, or a busy week. That vagueness is part of why it goes undetected, especially when a serum test waves it through.

The signs also tend to progress. A mild shortfall feels different from a deeper one, and recognizing the early signals is what gives you the chance to act before they worsen.
Early symptoms versus advanced symptoms
Early on, the NIH lists loss of appetite, nausea, fatigue, and general weakness. None of these screams “magnesium,” which is exactly the problem. They blend into ordinary tiredness.
As a shortfall deepens, the symptoms get harder to ignore: numbness and tingling, muscle contractions and cramps, abnormal heart rhythms, and in severe cases seizures or coronary spasms. A serious deficiency can also drag down calcium and potassium levels, since magnesium helps regulate both.
Across the patients we serve, the most common trio that prompts a magnesium question is cramping, palpitations, and poor sleep, often together. None of these confirms a deficiency on its own, but the pattern is a reasonable reason to look closer with the right test.
What quietly drains your magnesium
Diet is the biggest driver, but several everyday factors accelerate losses. Certain medications top the list. Acid reducers known as proton pump inhibitors, taken long term for reflux, and diuretics prescribed for blood pressure both increase magnesium loss over time.
Health conditions matter too. Type 2 diabetes raises the magnesium flushed out in urine, and gut conditions like Crohn’s disease, celiac disease, and chronic diarrhea cut how much you absorb from food. Heavy alcohol use compounds both problems.
Age and lifestyle round it out. Absorption tends to decline as people get older, and chronic stress and high caffeine intake nudge losses upward. Our lab partners report that people stacking two or three of these factors are the ones whose serum stays normal while their stored magnesium slips.
Why This Difference Matters for Americans
This isn’t a niche concern. Magnesium shortfall is widespread in the United States, and the standard test is the one most likely to overlook it. That combination is why so many people feel dismissed by a normal result.
The American diet leans heavily on processed and refined foods, which lose much of their magnesium during manufacturing. Pair that with depleted soil and lower intake of leafy greens, beans, nuts, and whole grains, and you get a population that’s chronically under-supplied.
The magnesium shortfall in the US diet
National survey data tell the story plainly. Roughly 48% of the US population takes in less magnesium from food than the requirement, based on NHANES dietary analysis. The NIH Office of Dietary Supplements notes that many Americans simply don’t get the recommended amount, with older men and teens among the most likely to fall short.
The adult RDA sits at 310 to 420 mg per day, varying by age and sex. Hitting that target through a typical fast-food-and-cereal diet is harder than it sounds, which is part of why intracellular shortfalls are common even in people who look healthy on paper.
The data below put the scale of the gap in context, with sources noted inside the table.
| Statistic | Figure | Source |
| US population below the required magnesium intake from food | About 48% | NHANES / Am J Clin Nutr |
| Total body magnesium found in blood serum | About 1% | Institute of Medicine |
| Enzyme reactions that require magnesium | 300+ | Institute of Medicine / NIH ODS |
| Adult RDA for magnesium | 310 to 420 mg/day | NIH Office of Dietary Supplements |
| Lower sudden cardiac death risk in the highest serum-magnesium quartile | 38% | ARIC cohort (via NIH ODS) |
| Filtered magnesium reabsorbed by the kidneys during shortage | More than 80% | NHANES-based research |
That figure on sudden cardiac death is a useful reminder that magnesium status isn’t cosmetic. In the Atherosclerosis Risk in Communities study cited by the NIH, people in the top range of serum magnesium had a markedly lower risk of sudden cardiac death than those at the bottom. Knowing your true magnesium status, not just a borderline-normal snapshot, has real stakes.
Normal Ranges and What Your Number Means
Reference ranges are where a lot of confusion starts, because the numbers for serum and RBC look nothing alike, and different labs print different RBC ranges. Understanding why clears up most of the worry.
Serum and RBC values aren’t on the same scale. Red blood cells concentrate magnesium, so an RBC result will always read higher than a serum result. A “4” on an RBC report and a “2” on a serum report can both be perfectly normal; they’re measuring different compartments.
Standard lab reference ranges (Quest, LabCorp)
For serum magnesium, the long-standing normal range is about 1.8 to 2.3 mg/dL, per the Institute of Medicine. Most labs use something close to this.
For RBC magnesium, the ranges differ by provider. Quest Diagnostics reports roughly 4.0 to 6.4 mg/dL, while LabCorp uses about 3.7 to 7.0 mg/dL. Many independent labs publish 4.2 to 6.8 mg/dL. The spread looks alarming until you know the reason behind it.
These ranges are built from population data, not from outcomes. A lab takes blood from a large sample of “healthy” people and sets the normal band around the middle 95%. If a big share of that sample is already low on magnesium, the so-called normal range reflects a population that’s broadly under-supplied to begin with.
Standard range versus functional/optimal targets
Some practitioners argue for tighter “functional” or “optimal” targets, often citing the upper half of the standard range as the goal. The logic is that simply avoiding the abnormal cutoff isn’t the same as having enough for your enzymes to run well.
There’s a caution worth stating clearly. These optimal targets come from clinical opinion and emerging research, not from formal outcome trials, and they aren’t standardized across labs. In cases reviewed by our medical team, the practical takeaway is to read your number against your own lab’s range first, then discuss any low-normal result with your clinician rather than self-diagnosing from a chart online.
A result near the bottom of the range deserves a conversation, especially alongside symptoms. A result comfortably in the middle is generally reassuring. Either way, the number is one input, not a verdict.
When to Choose an RBC Test Over a Serum Test
Most people don’t need an RBC magnesium test. For a routine checkup with no symptoms, serum is fine. The RBC test becomes worthwhile when there’s a specific reason to suspect a hidden shortfall, or when a normal serum result hasn’t matched how you feel.
The clearest signal is the mismatch itself: persistent symptoms with a normal serum magnesium. Beyond that, certain medications and conditions are known to drain magnesium, and the NIH lists the higher-risk groups directly.
| Scenario | What It May Suggest | Recommended Action |
| Normal serum magnesium but ongoing cramps, fatigue, or palpitations | A cellular shortfall the serum test missed | Ask your clinician about an RBC magnesium test |
| Long-term use of acid reducers (PPIs) or diuretics | Higher risk of magnesium loss | Consider RBC testing and review medications with your clinician |
| Type 2 diabetes or insulin resistance | Increased urinary magnesium loss | An RBC test gives a clearer status read |
| Gut conditions (Crohn’s, celiac, chronic diarrhea) | Reduced magnesium absorption | RBC test plus a full clinical work-up |
| Heavy or chronic alcohol use | Depleted magnesium stores | RBC test and medical guidance |
| Tracking a magnesium supplement plan | Need to confirm cells are actually responding | Repeat an RBC test after 8 to 12 weeks |
Who benefits most from the RBC test
People taking proton pump inhibitors for reflux, or loop and thiazide diuretics for blood pressure, lose magnesium at higher rates over time. So do people with poorly controlled diabetes, since elevated blood sugar increases magnesium flushed out in urine.
Anyone with a malabsorptive gut condition, from Crohn’s disease to celiac disease to chronic diarrhea, struggles to pull magnesium from food. Heavy alcohol use compounds the problem by accelerating urinary losses. Older adults round out the list, since absorption tends to decline with age.
If you fall into one of these groups and feel persistently off, an RBC magnesium test is a reasonable thing to raise with your doctor. Our lab partners report that this is precisely the population the test serves best, because their serum levels often stay normal while their reserves quietly slip.
How to Get Tested and Prepare
The RBC magnesium test isn’t included in a standard metabolic panel, so you have to request it specifically. Your doctor can add it to a blood draw, or you can order it directly through many consumer lab services in the US.
The logistics are straightforward, though a few details trip people up. Knowing them ahead of time saves a repeat draw.
Ordering, cost, insurance, and turnaround
Out of pocket, the RBC magnesium test commonly runs about $25 to $80, with many direct-access options landing in the $29 to $49 range. Insurance coverage varies; because it’s a specialty add-on rather than a routine screen, some plans won’t cover it without a documented reason, so it’s worth checking first.
No fasting is typically required. The blood is drawn into a specific tube (often a royal blue, lavender, or green top), then spun and separated promptly so only the red cells go to the analyzer. Results usually come back in about 5 to 7 business days, though sendout labs can take longer.
Patients commonly ask us whether they should pause supplements before testing. That’s a question for the ordering clinician, since the right answer depends on whether you’re establishing a baseline or checking how well a supplement is working.
Reading your result and what to do next
When the result arrives, compare it to your own lab’s printed range, not a number you read elsewhere. A value mid-range is generally reassuring. A value near or below the bottom, especially with symptoms, is worth acting on.
Across the patients we serve, the most common follow-up question is what to do with a low-normal number. The honest answer is that it depends on your symptoms, medications, and overall picture, which is why the next step is a conversation with your clinician rather than a guess.
If you’re using the test to track a supplement plan, retesting after roughly 8 to 12 weeks shows whether your cells are actually taking the magnesium up. That feedback loop is one of the test’s most practical uses.
Rebuilding magnesium through food and supplements
Food is the foundation, and the NIH points to leafy greens like spinach, legumes, nuts, seeds, whole grains, and some fortified cereals as reliable sources. Building these into regular meals raises stored magnesium gradually, which is usually the safest route.
When food isn’t enough, supplements come into play, ideally under medical guidance. The NIH notes that more easily absorbed forms include magnesium citrate, aspartate, lactate, and chloride. Some forms used in laxatives and antacids are less efficient for raising levels.
One safety note worth respecting: the upper limit for magnesium from supplements and medications is 350 mg per day for adults, and higher doses commonly cause diarrhea, nausea, and cramping. People with reduced kidney function need extra caution, since the kidneys clear excess magnesium, so any supplement plan in that situation belongs with a doctor.
Limitations: What Neither Test Can Tell You
It’s tempting to crown the RBC test the definitive answer, but that overstates the case. RBC magnesium is more informative than serum for chronic shortfalls, yet it still doesn’t capture the full picture.
Most of your magnesium is stored in bone and muscle, and no routine blood test measures those reserves directly. Red blood cells are a better window than plasma, not a complete one. A normal RBC result reduces the odds of a meaningful deficiency, but it can’t rule out every tissue-level shortfall.
There’s also variability between labs and methods, which is why two reports can read slightly differently. Our medical reviewers treat magnesium status as a judgment built from several inputs: your test result, your symptoms, your diet, your medications, and your medical history. The number guides the conversation; it doesn’t end it. Used that way, the RBC magnesium test is a genuinely useful tool, just not a crystal ball.
Frequently Asked Questions
What does an RBC magnesium test check?
It checks how much magnesium is stored inside your red blood cells, which reflects your tissue-level magnesium supply. Unlike a serum test that samples circulating magnesium, the RBC version looks at a stored pool, giving a steadier read on whether your body has enough magnesium over time rather than at a single moment.
How is RBC magnesium different from serum magnesium?
Serum magnesium measures the mineral circulating in your blood plasma, about 1% of body stores. RBC magnesium measures the supply inside your red blood cells, which runs roughly three times higher in concentration. Serum reflects the present moment; RBC reflects stored status, so it catches chronic shortfalls that serum often misses.
Is the RBC magnesium test more accurate than serum?
For detecting a chronic, low-grade shortfall, yes, the RBC test is generally more sensitive because it reads stored magnesium rather than the tightly regulated blood level. For acute swings or routine screening, serum works well. Neither is perfect, since most magnesium sits in bone and muscle that no blood test measures directly.
What is a normal RBC magnesium level?
Normal RBC magnesium is typically about 4.0 to 6.8 mg/dL, though the exact range depends on the lab. Quest Diagnostics reports roughly 4.0 to 6.4 mg/dL and LabCorp about 3.7 to 7.0 mg/dL. Always compare your result to the reference range printed on your own lab report.
Can serum magnesium be normal if I’m deficient?
Yes, and this is common. Your body pulls magnesium from cells and bone to keep blood levels steady, and your kidneys conserve magnesium during a shortage. As a result, serum can stay in the normal range while your cellular reserves run low, which is exactly why a normal serum result can be misleading.
How much does an RBC magnesium test cost without insurance?
Out of pocket, the test usually costs about $25 to $80, with many direct-access lab options in the $29 to $49 range. Pricing varies by lab and location. Because it’s a specialty add-on rather than a routine screen, comparing prices across providers before ordering is worth the few minutes.
Does insurance cover the RBC magnesium test?
Coverage varies by plan. Since the RBC magnesium test isn’t part of a standard panel, some insurers won’t cover it without a documented medical reason from your clinician. Check with your insurer or lab before testing, and ask your doctor whether your symptoms or medications justify coverage.
Where can I get an RBC magnesium test?
You can get it through your doctor, who can add it to a blood draw, or order it directly through many US consumer lab services that use Quest or LabCorp collection sites. The test isn’t part of routine panels, so you’ll need to request it by name when scheduling.
How long do results take?
Most RBC magnesium results come back within about 5 to 7 business days. Some labs that send the sample to a specialized reference facility can take longer, occasionally up to two to three weeks. Your ordering lab can give you a specific turnaround estimate when you book the draw.
What sample or tube is used?
The test uses whole blood collected in a specific tube, often a royal blue, lavender, or green top. The lab then spins the sample and separates the red cells from the plasma, usually within about two hours, and measures the magnesium inside the cells. This prompt handling keeps the result accurate.
Can diet alone fix a low RBC magnesium result?
Often it helps significantly. Magnesium-rich foods like leafy greens, legumes, nuts, seeds, and whole grains rebuild stores over time. For larger shortfalls, or when medications or gut conditions are draining magnesium, your clinician may recommend supplements. Retesting after 8 to 12 weeks shows whether your cellular levels are actually improving.
Medical disclaimer: This article is for general information and education only and isn’t a substitute for professional medical advice, diagnosis, or treatment. Reference ranges, costs, and coverage vary by lab and plan. Always talk with a qualified healthcare provider before ordering tests, interpreting results, or starting any supplement, especially if you take prescription medications or have a chronic condition.
References
- National Institutes of Health, Office of Dietary Supplements: Magnesium (Health Professional Fact Sheet)
- National Institutes of Health, Office of Dietary Supplements: Magnesium (Consumer Fact Sheet)
- Institute of Medicine, Dietary Reference Intakes for Calcium, Phosphorus, Magnesium, Vitamin D, and Fluoride (NCBI Bookshelf)
- LabCorp: Magnesium, RBC (Test 080283)
- Suboptimal Magnesium Status in the United States (American Journal of Clinical Nutrition, PubMed)
- Magnesium Deficiency Prevalence Analysis Using NHANES Data (PMC)
- Interpreting Magnesium Status to Enhance Clinical Care (PMC)





