
A routine blood test comes back, and one line stands out: your RBC count is high. Unlike a low count that screams fatigue, a high one often whispers, hiding behind no symptoms at all while quietly thickening your blood. That silence is exactly why understanding the result matters.
Table of Contents
Quick Answer: A high RBC count means your blood holds more red blood cells than normal, a condition called erythrocytosis or polycythemia. Extra red cells thicken the blood, which can slow circulation and raise the risk of clots. Common causes are harmless, like dehydration, smoking, or high altitude, but a persistent high count can signal lung, heart, or bone marrow conditions. It’s found on a complete blood count (CBC), and treatment depends on the cause.
At a Glance
- A high RBC count, or polycythemia, means too many red blood cells, which makes blood thicker and slower.
- The three categories are relative (dehydration), secondary (low oxygen or hormones), and primary (a marrow disorder).
- Dehydration, smoking, and high altitude are the most common and least worrying causes.
- The main risk of a truly elevated count is dangerous blood clots, including stroke and heart attack.
- Many people have no symptoms, so a high count is often caught by chance on routine bloodwork.
- The right treatment, from hydration to phlebotomy, depends entirely on the underlying cause.
What Is a High RBC Count?
A high RBC count means a blood sample holds more red blood cells than the normal reference range for your age and sex. Red blood cells, or erythrocytes, carry oxygen from your lungs to every tissue.
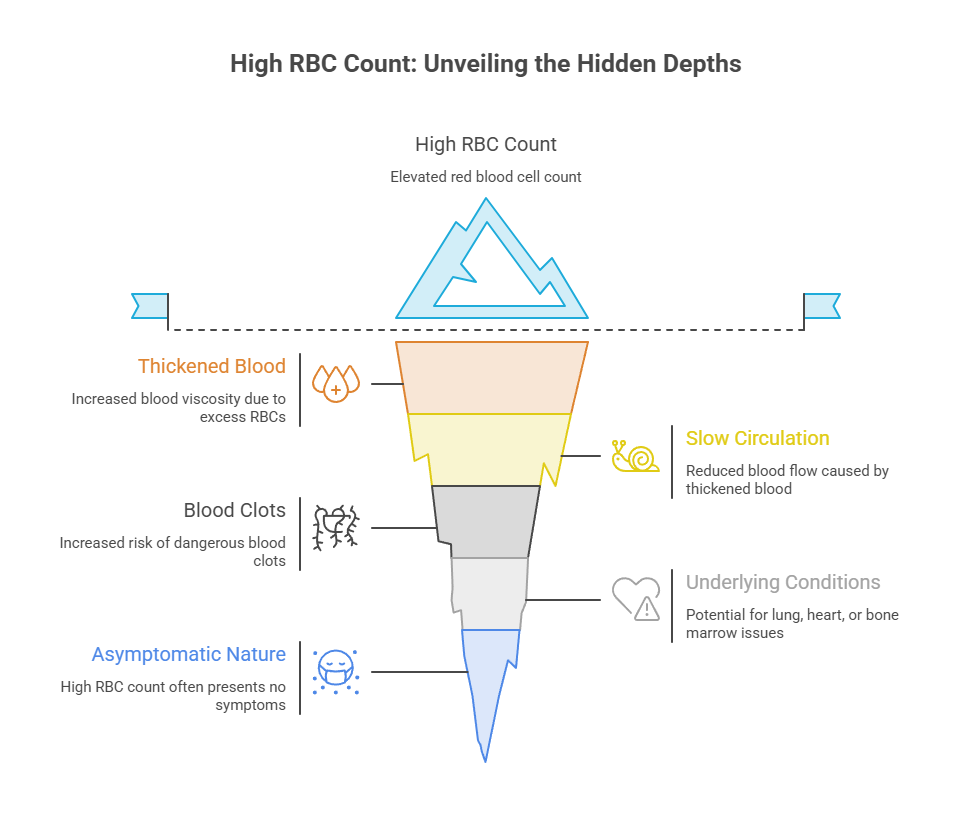
When there are too many, the blood grows thicker and more viscous, which can slow its flow through small vessels. Extra red blood cells thicken your blood and raise the risk of clots, which is the core concern behind an elevated count.
The pace of red cell production is set by erythropoietin (EPO), a hormone your kidneys release when they sense low oxygen. Patients booking a CBC through HealthCareOnTime often see RBC flagged with an H and want to know whether it’s a quirk or a warning.
High RBC Count vs Polycythemia vs Erythrocytosis
These words get used interchangeably, and the overlap is mostly fair. Erythrocytosis means a raised red blood cell count or red cell mass, while polycythemia is the broader term for thickened blood from too many cells.
In everyday lab talk, a high RBC count, erythrocytosis, and polycythemia all point to the same finding. The important split is what’s driving it, not which label appears on the report.
Doctors sort the cause into three buckets, relative, primary, and secondary. Our medical reviewers stress that this distinction, not the raw number, shapes what happens next.
How High Is Too High? Normal vs High Ranges
Reference ranges vary slightly by lab, so always compare your result to the range printed on your own report. A high RBC count means more red cells than the typical range, which is 4.7 to 6.1 million cells per microliter for men and 4.2 to 5.4 million for women.
So a count above roughly 6.1 million in men or 5.4 million in women is generally flagged as high. Doctors also read hemoglobin and hematocrit, since those usually rise together with a high RBC count.
For the specific diagnosis of polycythemia vera, the thresholds are higher. Erythrocytosis defined as hemoglobin above 16.5 g/dL in men or above 16.0 g/dL in women is a required diagnostic criterion.
| Group | Normal RBC (million cells/uL) | Normal Hemoglobin (g/dL) | High RBC (above) | High Hematocrit (above) |
| Adult men | 4.7 to 6.1 | 13.5 to 17.5 | 6.1 | 49% |
| Adult women | 4.2 to 5.4 | 12.0 to 15.5 | 5.4 | 48% |
| Children (school age) | 4.0 to 5.5 | 11.5 to 15.5 | 5.5 | 45% |
| Adults 65 and older | 4.2 to 5.8 | 12.0 to 17.0 | 5.8 | 49% |
| Polycythemia vera flag | n/a | Men above 16.5, women above 16.0 | n/a | Men 49%, women 48% |
What a High RBC Count Means for Your Body
A high RBC count is a clue, not a verdict. It tells your doctor that either your body is making too many red cells or your plasma volume has dropped, then points toward why.
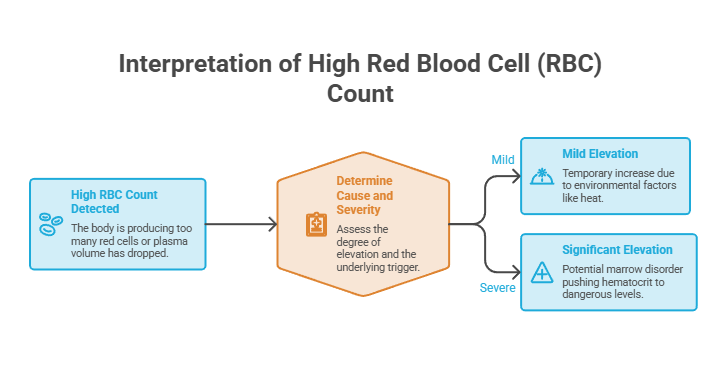
What it means for you depends on how high the count is and what’s causing it. A mildly raised number from a hot afternoon is worlds apart from a marrow disorder pushing your hematocrit toward dangerous territory.
Why Thicker Blood Raises Clot Risk
Blood is a balance of cells and fluid. Pack in too many red cells, and the mixture turns syrupy, which makes it harder to push through narrow vessels and easier to clot.
If you have a high red blood cell count, you have erythrocytosis, which makes your blood thicker than it should be and could increase your risk for blood clots. Those clots can trigger a stroke, a heart attack, or a clot in the legs or lungs.
In cases reviewed by our medical team, the danger rarely comes from the number itself but from what thick blood does downstream. That’s why a persistent high count earns a careful workup.
When It’s Harmless and When It’s Not
Plenty of high counts are benign and temporary. A relative rise from dehydration corrects itself once you rehydrate, and an altitude-driven bump is a normal adaptation. A high count after a few days of vomiting or a stomach bug usually fades as fluids return.
The picture changes when the count stays high without an obvious reason. A high red blood cell count can be a sign of a disease or disorder, though it doesn’t always mean you have a health problem.
The serious end is polycythemia vera, a bone marrow cancer where clot risk is real. Thrombotic events are the most frequent complication of PV, affecting 39 to 41 percent of patients. Across patients we serve, that statistic is the reason we never wave off a stubbornly high reading.
Common Causes of a High RBC Count
Nearly every high RBC count falls into one of three categories. Either your plasma volume dropped (relative), an outside signal is driving production (secondary), or your marrow is overproducing on its own (primary).
Sorting which category applies is how doctors move from your count is high to a plan that fits. Our medical team works the cause first, never the number in isolation.
Relative (Apparent) High RBC: Dehydration and Plasma Loss
The simplest cause of a high RBC count isn’t extra red cells at all, it’s less fluid. When plasma volume falls, the same number of red cells looks concentrated, so the count reads high.
Dehydration is the classic trigger, whether from heat, illness, hard exercise, or diuretic medications. When the body lacks adequate water, the blood concentrates and the red blood cell count rises.
This relative or apparent polycythemia usually resolves with rehydration. Our lab partners often suggest rechecking a borderline-high result after a day or two of steady fluids before any deeper testing.
Secondary Causes: Low Oxygen, Smoking, and EPO
Secondary polycythemia is real overproduction, driven by extra erythropoietin. Most often, the body is reacting to low oxygen by making more red cells to carry it.
This is an appropriate response that has gone slightly overboard, and it points to whatever is limiting oxygen. The list of secondary triggers is long but well understood.
Lung Disease, Sleep Apnea, and Altitude
Anything that lowers your blood oxygen can push red cell production up. Chronic obstructive pulmonary disease, sleep apnea, and high-altitude living can increase red blood cell production to improve oxygen transport.
Living above 5,000 feet routinely raises counts by 5 to 10 percent, a normal adaptation to thinner air. Sleep apnea is a frequently missed culprit, since the repeated nighttime oxygen dips quietly drive the marrow.
Carbon monoxide from smoking does something similar. Carbon monoxide from smoking binds to hemoglobin, reducing oxygen delivery and stimulating red blood cell production as compensation.
Testosterone Therapy and Performance Drugs
A fast-growing cause in the US is testosterone replacement therapy. Testosterone stimulates red cell production, so a rising hematocrit is one of the most common side effects providers monitor.
Dehydration can also temporarily elevate hematocrit in people on testosterone, since less plasma volume raises the proportion of red cells. Anabolic steroids and injected EPO used for doping raise counts the same way.
Patients commonly ask us whether their TRT explains a flagged count, and often it does. The fix is usually a dose adjustment or scheduled blood removal, guided by the prescribing clinician.
EPO-Secreting Tumors
Less commonly, a tumor itself pumps out erythropoietin and drives the count up. Certain cancers, especially kidney and liver cancers, can secrete erythropoietin, stimulating red blood cell production.
These cases are uncommon but important, which is why an unexplained high count sometimes prompts kidney imaging. Benign kidney cysts and, rarely, certain uterine or liver growths can also raise erythropoietin. The reassuring context is that tumor-driven counts are far rarer than dehydration or smoking.
Primary Cause: Polycythemia Vera
Primary polycythemia means the marrow overproduces red cells on its own, independent of EPO. The main example is polycythemia vera (PV), a chronic blood cancer.
More than 95 percent of PV patients carry a JAK2 gene variant, which helps distinguish PV from secondary causes of erythrocytosis such as tobacco smoking or sleep apnea. That genetic signature is central to diagnosis.
PV tends to appear later in life. It is the most common myeloproliferative neoplasm, with a mean age at diagnosis of about 60, and it occurs more often in men.
| Type | What’s Happening | EPO Level | Typical Causes |
| Relative (apparent) | Plasma volume drops, cells concentrate | Normal | Dehydration, diuretics, hard exercise |
| Secondary (absolute) | EPO drives real overproduction | Normal or high | Lung disease, sleep apnea, altitude, smoking, TRT, EPO-secreting tumors |
| Primary (absolute) | Marrow overproduces on its own | Low | Polycythemia vera (JAK2 variant) |
Polycythemia vera is uncommon but not rare. PV affects approximately 65,000 people in the US, with an annual incidence of 0.5 to 4.0 cases per 100,000 persons. In cases seen across our diagnostic network, it’s the diagnosis doctors most want to confirm or rule out when a high count has no obvious explanation.
Symptoms of a High RBC Count
Here’s the tricky part: a high RBC count often causes nothing you’d notice. Many people feel completely fine and only learn of it through routine labs.
When symptoms do appear, they come from thicker blood moving sluggishly and delivering oxygen less efficiently. The signs cluster into common symptoms, PV-specific clues, and urgent clot warnings.
Early and Common Symptoms
As counts climb, the first symptoms are usually vague and easy to attribute to something else. A mildly elevated count often produces no symptoms, but as counts climb higher, thicker blood circulates less efficiently and you might notice headaches, dizziness, fatigue, or blurred vision.
Other common signs include a flushed or reddish complexion, shortness of breath, and joint pain. Symptoms of a high RBC count include headaches, dizziness, blurred vision, and a flushed or reddish skin tone, with itching, fatigue, and joint pain also possible.
Nosebleeds, numbness or tingling, and ringing in the ears can also show up. Our medical reviewers note that because these overlap with many conditions, the CBC is what ties them together.
Symptoms Specific to Polycythemia Vera
Polycythemia vera carries a few telltale signs that point beyond a simple high count. The most recognizable is itching after contact with warm water.
Itching after a warm bath or shower is a classic sign of PV, caused by certain immune cells in the skin reacting to heat. This aquagenic pruritus is distinctive enough to prompt testing.
Other PV features are well documented. Patients may have pruritus in about 33 percent, erythromelalgia (burning, red hands or feet) in roughly 5 percent, transient visual changes in about 14 percent, and an enlarged spleen in around 36 percent with abdominal discomfort.
Warning Signs of a Blood Clot (Urgent)
Because thick blood clots more easily, certain symptoms demand immediate care. These are signals not to wait for a scheduled appointment.
Seek emergency help for sudden chest pain or pressure, shortness of breath, weakness or numbness on one side, slurred speech, vision loss, or a severe headache. Swelling, warmth, or pain in one leg can signal a deep vein clot.
In cases reviewed by our medical team, people with very high counts are urged to treat these red flags as emergencies. Prompt action can be the difference in a stroke or heart attack.
How a High RBC Count Is Diagnosed
Diagnosis starts with the same CBC that flagged the count, then adds targeted tests to find the cause. The goal is to confirm a true rise and sort primary from secondary.
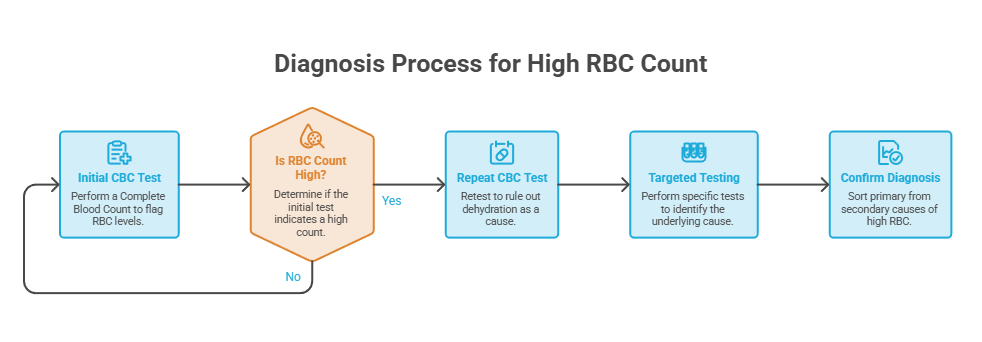
A high RBC count on one test is sometimes just dehydration, so doctors often repeat it. No fasting is needed for a CBC, and a basic panel runs modestly, often around $29 at major labs, so confirming the result is rarely a barrier.
The CBC, Hemoglobin, and Hematocrit
The CBC reports the red cell count alongside hemoglobin and hematocrit, and these three usually move together. Tests to determine how many red blood cells are in your blood include the red blood cell count, hemoglobin, hematocrit, and the complete blood count.
Hematocrit, the percentage of blood made up of red cells, is especially useful for tracking thickness and clot risk. A markedly high hematocrit is what often triggers treatment.
Doctors also look at the white cell and platelet counts, since polycythemia vera frequently raises those too. Our lab partners report that the full CBC pattern often hints at the cause before any specialized test.
EPO and JAK2 Testing (primary vs secondary)
Two tests separate the categories. An erythropoietin level distinguishes a marrow problem from an oxygen-driven one, and a JAK2 test checks for the PV mutation.
The EPO contrast is striking. In PV, EPO tends to run low because the marrow overproduces on its own, while in secondary causes EPO is usually normal or high, with one study showing average EPO around 3.4 mIU/mL in PV patients versus 23.7 mIU/mL in secondary cases.
If PV is suspected, further steps follow. Additional tests may include a bone marrow biopsy to check for abnormal cell growth and an erythropoietin level to determine whether there’s overproduction of EPO.
| US Statistic | Figure | Source |
| People with polycythemia vera in the US | About 65,000 | JAMA review, 2024 |
| PV prevalence | 44 to 57 per 100,000 | MedlinePlus, NIH |
| PV annual incidence | 0.5 to 4.0 per 100,000 | JAMA review, 2024 |
| PV patients carrying a JAK2 variant | Over 95% | JAMA review, 2024 |
| PV patients with thrombotic events | 39% to 41% | Therapeutic Advances in Hematology, 2025 |
| Itching (pruritus) in PV patients | About 33% | JAMA review, 2024 |
How to Lower a High RBC Count
Lowering a high RBC count is not about a single trick, it’s about correcting what’s driving it. The right approach depends on whether the cause is dehydration, low oxygen, hormones, or a marrow disorder.
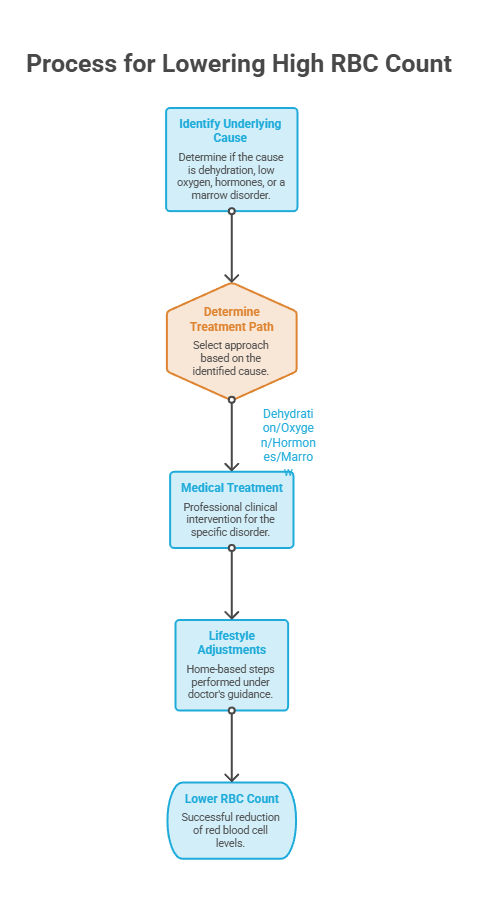
That said, several proven steps help, and some you can start at home with your doctor’s guidance. Lifestyle moves support medical treatment rather than replacing it.
Treat the Underlying Cause First
If low oxygen is fueling the count, the fix targets the oxygen problem, not the blood. Treatment of secondary polycythemia depends on its cause, with supplemental oxygen for chronic hypoxia and therapies directed at the underlying condition, such as treating heart failure or chronic lung disease.
Treating sleep apnea, often with a CPAP machine, can bring an oxygen-driven count back down. Managing COPD or heart disease does the same by restoring better oxygen delivery.
This is why our medical team insists on a diagnosis before a plan. Removing blood from someone whose high count is compensating for low oxygen can occasionally do more harm than good.
Hydration, Quitting Smoking, and Lifestyle
For relative polycythemia, fluids are the answer. Staying hydrated keeps blood volume balanced, since dehydration can falsely elevate RBC counts, and quitting smoking helps normalize oxygen flow and red cell production.
Be realistic about what water can do, though. Hydration can reduce relative elevations caused by low plasma volume, but it won’t significantly lower a high count from excess red blood cell production.
Quitting smoking is one of the highest-impact moves for a smoking-related count. Moderate exercise supports circulation, while extreme endurance training can temporarily nudge counts up. Cutting back on alcohol and treating any sleep problems round out the everyday steps worth taking.
Therapeutic Phlebotomy and Medication
When a count is dangerously high, doctors remove blood directly. Phlebotomy lowers the hematocrit to normal levels by drawing blood out, often around 500 milliliters in one visit.
For polycythemia vera, medication is added. A provider may prescribe hydroxyurea to slow the body’s production of red blood cells, and people with PV often undergo routine therapeutic phlebotomy to keep the count under control.
Low-dose aspirin is common too. Aspirin is used in PV to lower the risk of clotting events, usually alongside phlebotomy, though it’s generally avoided in people with a bleeding history. With phlebotomy, many PV patients lead normal lives and enjoy a normal life expectancy.
Managing TRT-Related High Counts
Testosterone-related rises have their own playbook. For TRT patients, a provider may lower the dose or switch the delivery method to reduce red blood cell stimulation, and managing sleep apnea helps too.
Scheduled blood removal works well here. In one review, 85 percent of people who received therapeutic phlebotomy for secondary polycythemia said their symptoms improved.
Donating blood at a center is another option some men use, with a clinician’s blessing. Our medical reviewers caution that removing blood too often can deplete iron, so the schedule should be doctor-guided.
| Scenario | What It May Mean | Recommended Action |
| Slightly high RBC after a hot day or workout | Probable dehydration | Rehydrate, repeat the test in a week |
| High RBC with heavy smoking | Smoking-related secondary | Quit smoking; recheck after several weeks |
| High RBC, loud snoring, daytime sleepiness | Possible sleep apnea | Ask your doctor about a sleep study |
| High RBC on testosterone therapy | TRT-related rise | Discuss dose, hydration, and possible phlebotomy |
| High RBC with itching after showers, ruddy skin | Possible polycythemia vera | Request EPO and JAK2 testing |
| Sudden chest pain, leg swelling, or vision loss | Possible blood clot | Seek emergency care now |
When to See a Doctor
A high RBC count on routine labs is a reason to follow up, not to panic. The timing depends on your symptoms and how high the number is.
A single mildly high reading often just needs a recheck after hydration. A persistent or markedly high count, or any worrying symptom, deserves prompt evaluation.
Red-Flag Symptoms That Need Urgent Care
Some situations call for same-day or emergency attention. Don’t wait if these appear.
Seek urgent care for chest pain, sudden shortness of breath, one-sided weakness or numbness, slurred speech, vision loss, a severe headache, or a swollen, painful leg. Coughing up blood or sudden, sharp pain when breathing can point to a clot in the lungs. These can signal a clot, stroke, or heart event.
People with known heart or lung disease should treat new symptoms more cautiously. In cases reviewed by our medical team, fast action on these signs prevents serious complications.
Questions to Ask Your Doctor
A few focused questions turn a confusing result into a clear plan. Bring them to your visit.
Ask whether your hemoglobin and hematocrit are also high, whether dehydration could explain it, and whether you need EPO and JAK2 testing. Then ask what’s driving your count and whether treatment is needed.
It’s also fair to ask whether smoking, sleep apnea, medications, or testosterone therapy could be contributing. Patients who arrive with these questions tend to leave with a much clearer path forward.
Frequently Asked Questions
What is considered a high RBC count?
A high RBC count generally falls above about 6.1 million cells per microliter for men and 5.4 million for women, though labs differ slightly. Doctors also weigh hemoglobin and hematocrit. Compare your result to your report’s reference range, since a single high reading may simply reflect dehydration.
What is the most common cause of a high RBC count?
Dehydration is the most common and least worrying cause, since less plasma makes red cells look concentrated. Smoking and high-altitude living are also frequent. Persistent elevation can point to lung disease, sleep apnea, testosterone therapy, or, less often, the bone marrow disorder polycythemia vera.
What are the symptoms of a high red blood cell count?
Many people have no symptoms. When they appear, common ones include headaches, dizziness, fatigue, blurred vision, a flushed or reddish complexion, and itching after a warm shower. Thicker blood can also cause shortness of breath, joint pain, nosebleeds, or tingling as counts climb higher.
Is a high RBC count dangerous?
It can be, mainly because thicker blood raises the risk of clots, stroke, and heart attack. Mild, temporary rises from dehydration or altitude are usually harmless. A persistent or very high count, especially with hematocrit elevation, needs evaluation and sometimes treatment to lower clot risk.
Can dehydration cause a high RBC count?
Yes, and it’s the most common explanation. Dehydration reduces plasma volume, so the same number of red cells appears concentrated, producing a falsely high count called relative polycythemia. Rehydrating and repeating the test usually returns the number to normal without any further treatment needed.
Does a high RBC count mean cancer or leukemia?
Usually not. Most high counts trace to dehydration, smoking, altitude, lung conditions, or testosterone therapy. Polycythemia vera, a slow-growing blood cancer, is one serious cause, identified by a low EPO level and a JAK2 mutation. A persistent, unexplained high count deserves a proper workup, not assumption.
How do you lower a high RBC count?
Treat the cause first. Hydration fixes dehydration-driven counts, quitting smoking helps smoking-related ones, and treating sleep apnea or lung disease addresses oxygen-driven rises. For very high counts or polycythemia vera, doctors use therapeutic phlebotomy, low-dose aspirin, and sometimes hydroxyurea to reduce clot risk.
Can testosterone therapy raise my RBC count?
Yes. Testosterone stimulates red blood cell production, so a rising hematocrit and RBC count is one of the most common side effects of TRT. Providers monitor it routinely. Management may include adjusting the dose or delivery method, staying hydrated, and sometimes scheduled blood removal.
What is the difference between primary and secondary polycythemia?
Primary polycythemia means the bone marrow overproduces red cells on its own, as in polycythemia vera, where EPO is low. Secondary polycythemia is driven by an outside signal, usually extra EPO from low oxygen, smoking, or a tumor, where EPO runs normal or high.
Does smoking cause a high RBC count?
Yes. Carbon monoxide from cigarettes binds to hemoglobin and reduces oxygen delivery, so the body compensates by making more red blood cells. This smoking-related secondary polycythemia often improves after quitting, though it can take several weeks to months for counts to normalize.
What hematocrit level is considered dangerous?
There’s no single universal cutoff, since it depends on the cause, symptoms, and your health. Hematocrit above 49 percent in men or 48 percent in women is generally flagged, and doctors often treat polycythemia vera to keep it below about 45 percent. Very high levels raise clot risk and warrant prompt care.
Can a high RBC count return to normal?
Often, yes. Counts from dehydration, smoking, or temporary causes usually normalize once the trigger is addressed. Secondary counts improve when the underlying condition is treated. Polycythemia vera can’t be cured, but phlebotomy and medication keep counts controlled, and many people live normally for decades.
Medical Disclaimer: This article is for general educational purposes and does not replace professional medical advice, diagnosis, or treatment. Reference ranges and thresholds vary between laboratories, and only a qualified healthcare provider can interpret your results in context. Always consult your doctor about a high RBC count or symptoms, and seek emergency care for chest pain, sudden weakness, vision loss, or signs of a blood clot.
References
- MedlinePlus Genetics: Polycythemia Vera
- JAMA / NIH: Diagnosis and Treatment of Polycythemia Vera, A Review
- Merck Manual Professional Edition: Polycythemia Vera
- Cleveland Clinic: High Red Blood Cell Count
- eMedicineHealth: Polycythemia (High Red Blood Cell Count)
- Therapeutic Advances in Hematology: Disease Management in Adults With Polycythemia Vera





