
A healthy adult’s blood should contain exactly zero nucleated red blood cells. So when even one shows up on a report, it isn’t a rounding error. It’s your body waving a flag.
Table of Contents
That flag can mean something minor and temporary, or it can point to a condition that needs attention soon. The number matters, but so does the story around it.
Quick Answer: Nucleated red blood cells (NRBCs) are immature red blood cells that still contain a nucleus. In healthy adults they’re normally absent, reported as 0 per 100 white blood cells. Their presence usually signals that the bone marrow is under stress or working overtime, often from severe anemia, low oxygen, infection, or a marrow disorder. Newborns normally have some. Any finding in an adult deserves follow-up to find the cause.
At a Glance
- Mature red blood cells lose their nucleus before entering the bloodstream, so a circulating nucleated red cell is, by definition, immature.
- In healthy adults, the normal NRBC count is zero; even a small number is reported and investigated.
- Common reasons NRBCs appear include severe anemia, hemolysis, low oxygen, severe infection, and bone marrow disorders.
- Newborns normally have some NRBCs, which clear within the first weeks of life.
- In critically ill adults, higher NRBC counts are linked to worse outcomes, which is why hospitals track them.
- NRBCs are a clue, not a diagnosis; the underlying cause determines what happens next.
What Are Nucleated Red Blood Cells?
Nucleated red blood cells are red blood cells caught in an early stage of development, still carrying the nucleus they haven’t yet shed. Hematologists also call them normoblasts or erythroblasts.
Your bone marrow builds red blood cells in stages. As SelfDecode Labs explains, these cells normally live only in the marrow while they mature, and their presence in circulating blood is termed normoblastemia.
From Normoblast to Mature Red Cell
A red blood cell spends its early life packed with a nucleus that directs its growth. Before the cell graduates into the bloodstream, it ejects that nucleus.
Losing the nucleus isn’t a flaw; it’s the final step of maturity. It frees up space for more hemoglobin and lets the cell flex through the tiniest capillaries, which is exactly what efficient oxygen delivery requires.
Why They Normally Stay in the Bone Marrow
Healthy marrow acts like a gatekeeper, holding immature cells back until they’re ready. Only mature, nucleus-free red cells are meant to pass into circulation.
When NRBCs turn up in the blood, that gate has been pushed open, either by intense demand for new red cells or by a process disrupting normal production. Patients reviewing a CBC with us often ask why an immature cell ended up on their report, and that pushed-open gate is the short answer.
Other Names You’ll See
Lab reports and clinicians use a few terms interchangeably. Normoblast and erythroblast both refer to the nucleated red cell at various developmental stages.
On your results, the line usually reads “NRBC” or “nucleated RBC,” sometimes with both a percentage and an absolute number. Knowing these are the same thing keeps a report from looking more complicated than it is.
How NRBCs Show Up on a Blood Test
NRBCs are detected as part of a complete blood count, specifically the CBC with differential. According to HealthMatters.io, their appearance in a CBC is noteworthy because they usually don’t circulate in peripheral blood.
The result often needs to be requested or flagged, since many routine panels report it only when the cells are detected. That’s why a patient may see “NRBC” appear suddenly on one report and not on another.
NRBCs and the CBC With Differential
The CBC measures your red cells, white cells, and platelets. The differential breaks down the white cells and, when present, counts nucleated red cells separately.
Modern hematology analyzers can detect and tally NRBCs automatically. Our lab partners report that a flagged sample still gets a manual smear review, because a trained eye confirms the count and looks for the company those cells keep.
How They’re Measured
A drop of blood is run through an automated analyzer, and a stained smear is examined under a microscope when confirmation is needed. The smear also reveals related clues, like the shapes of the red cells or the presence of immature white cells.
This pairing matters more than it might seem. The analyzer provides speed and a number, while the smear provides the context that a number alone can’t give, including whether other abnormal cells are present.
Two Reporting Formats
One detail trips up a lot of people reading their own results, because NRBCs are reported in two ways that aren’t on the same scale.
The first is NRBCs per 100 white blood cells (a ratio, sometimes shown as a percentage). The second is an absolute count, the number of NRBCs per microliter of blood. Healthline notes an ideal result is 0.3 per 100 WBC (0.3%) or less, while hospital studies often track the absolute count per microliter, so the same patient can see two very different-looking numbers.
How the Nucleated RBC Test Is Done
As a rule, you don’t order an NRBC test on its own. It comes bundled with a complete blood count, the same routine blood draw used at most checkups, with the nucleated cell count reported when the lab detects or looks for it.
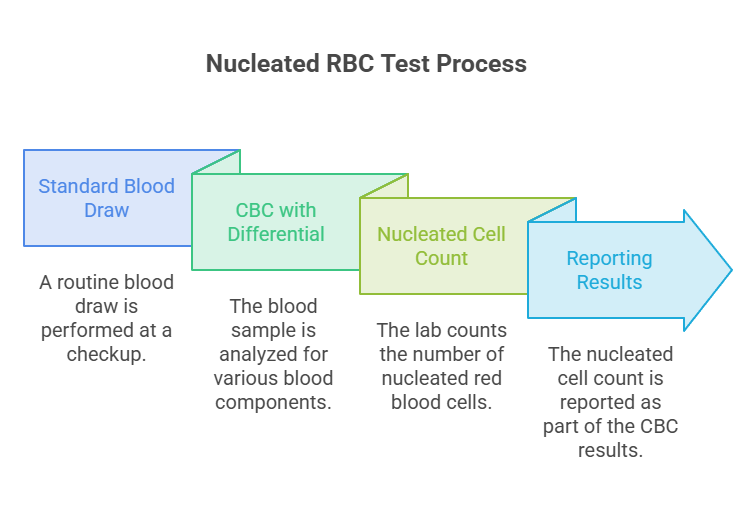
That means there’s nothing special to do on your end. The finding simply falls out of a standard CBC with differential.
The Blood Draw
A phlebotomist cleans a spot on your arm, applies a band to raise the vein, and draws a small sample into a tube. You may feel a brief pinch as the needle goes in and out.
The sample then travels to the lab, where an analyzer runs the count and a smear is reviewed if anything is flagged. Results are often back within a day, sometimes the same day.
Do You Need to Prepare?
For a standard CBC, no fasting is required, and you can eat and drink normally beforehand. Staying hydrated is still sensible for a comfortable, efficient draw.
If the CBC is bundled with other tests that require fasting, follow those instructions. Patients booking panels through HealthCareOnTime are told in advance when fasting applies, so always check your specific order.
What’s Normal vs Abnormal
For a healthy adult, the normal nucleated RBC count is zero. The body’s gatekeeping works so well that mature red cells alone reach the bloodstream.
Even a single NRBC per 100 white cells gets reported, because a small number can still carry meaning. The table below maps what different results tend to suggest.
| NRBC Result | Typical Meaning | Common Triggers | What It Suggests |
| 0 per 100 WBC (adults) | Normal | None | Healthy red cell maturation |
| Present in a newborn | Often normal | Birth and transition to breathing | Usually expected; clears within weeks |
| 1 to a few per 100 WBC | Mild, needs context | Recovering or mild anemia, recent stress | Worth a closer look and follow-up |
| Moderate elevation | Notable marrow response | Hemolysis, low oxygen, infection | Active demand or stress on the marrow |
| Marked elevation | Significant finding | Marrow infiltration, severe illness | Often serious; prompt evaluation |
Why Zero Is the Adult Baseline
A zero reading means your red cells are maturing properly before they enter circulation. That’s the expected, healthy state, and it’s why no number on this line is the goal.
Because the baseline is zero rather than a range, there’s no meaningful “low” NRBC in adults. In results reviewed across our diagnostic network, the question is almost always why any are present, not whether there are too few.
Newborns and Infants
Newborns are the big exception. A baby’s blood normally contains some NRBCs at birth, a leftover of the rapid red cell production of fetal life.
Healthline notes these cells disappear within the first few weeks of life. A higher-than-expected newborn count can suggest stress before or during birth, such as low oxygen or a hemolytic condition, and is interpreted by the pediatric team rather than read as an adult result would be.
Why Nucleated RBCs Appear (The Causes)
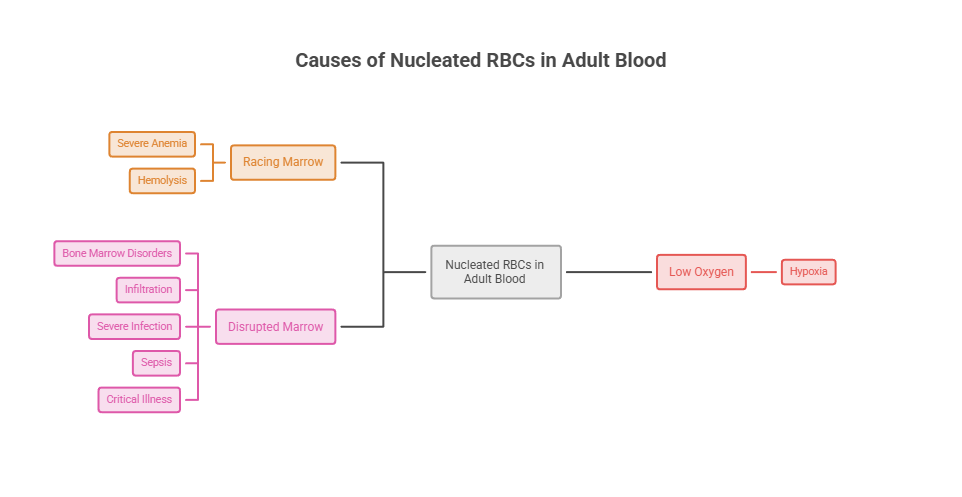
NRBCs in adult blood almost always trace to one of a few broad mechanisms. The marrow is either racing to replace red cells, responding to low oxygen, or being disrupted by disease.
Understanding which category you fall into is what turns a scary line on a report into a clear next step. Our medical reviewers note that the cause, far more than the number, shapes how worried anyone should be.
Severe Anemia and Hemolysis
When red cells are lost or destroyed faster than normal, the marrow goes into overdrive and may release immature cells early. Rapid blood loss does this, and so do hemolytic anemias, where red cells break down prematurely.
Inherited hemolytic conditions like sickle cell disease, thalassemia, and hereditary spherocytosis are classic triggers. Healthline notes that destruction of many red cells in a short time can drive a rapid jump in production, spilling NRBCs into the blood.
Low Oxygen (Hypoxia)
Your body responds to low oxygen by making more red cells, since red cells carry oxygen. That ramped-up production can push immature cells into circulation.
Chronic lung disease, certain heart conditions, and severe acute illness all lower oxygen delivery. Patients we serve with long-standing breathing conditions sometimes show NRBCs as a sign their marrow is straining to compensate.
Bone Marrow Disorders and Infiltration
Sometimes the marrow itself is the problem. Conditions that crowd, scar, or replace healthy marrow can break the barrier that normally holds immature cells back.
Leukemia, myelofibrosis, and cancer that has spread to the marrow are important examples. When NRBCs appear alongside immature white blood cells, the pattern is called a leukoerythroblastic reaction, a finding that raises concern for marrow infiltration and warrants prompt hematology evaluation.
Severe Infection, Sepsis, and Critical Illness
Serious, body-wide stress can also flush NRBCs into the blood. Severe infections trigger a strong inflammatory response, and critically ill patients often show NRBCs as part of that reaction.
Research points to inflammatory signals and low oxygen as the drivers. One COVID-19 ARDS study notes NRBC release is linked to inflammatory markers like interleukin-6 and to low oxygen levels, marking disturbed marrow function under stress.
What an Elevated NRBC Means for Prognosis
In the hospital setting, NRBCs have become a watched signal because their presence tracks with how sick a patient is. This is where the evidence is strongest, and where the thin biomarker pages stay quiet.
The figures below come from studies of critically ill adults. They don’t apply to a healthy person with a single NRBC on a routine panel, but they explain why clinicians take the finding seriously in serious illness.
| Setting | NRBC Finding | Outcome Association | Source |
| Septic ICU patients | Maximum 100/µL or higher | About 5x higher odds of death (OR 5.03) | Septic ICU study, 2025 |
| COVID-19 ARDS | Non-survivors 1,090/µL vs survivors 140/µL | Strongly linked to mortality | COVID ARDS study, 2024 |
| COVID-19 ARDS | Reaching 500/µL or higher | 3.2x higher long-term mortality (HR 3.2) | COVID ARDS study, 2024 |
| ARDS (general) | NRBC above 220/µL | Predicts ICU death | ARDS study, 2018 |
| Cardiac ICU | NRBCs present in 54.6% of patients | Predicts all-cause mortality | Cardiac ICU study |
Why NRBCs Track With Severity
The same forces that make someone critically ill also push NRBCs out of the marrow. Inflammation, low oxygen, and high erythropoietin levels appear together with their release.
A 2025 study of septic ICU patients found that a maximum NRBC of at least 100 per microliter was associated with roughly fivefold higher odds of death. A 2024 study of COVID-19 ARDS patients found non-survivors carried far higher NRBC levels than survivors.
Context Matters More Than the Number Alone
These prognostic numbers describe populations of very sick patients, not individuals reading a routine result. A high count in an ICU is a completely different situation than one NRBC on an outpatient CBC.
Patients commonly ask us whether a flagged NRBC means the worst. The honest answer is that the cause and the clinical picture decide everything, which is why the next step is always interpretation, never panic.
Symptoms That May Accompany Nucleated RBCs
NRBCs themselves don’t cause symptoms; they’re a sign of something else. So any symptoms you feel come from the underlying condition that’s driving the cells into your blood.
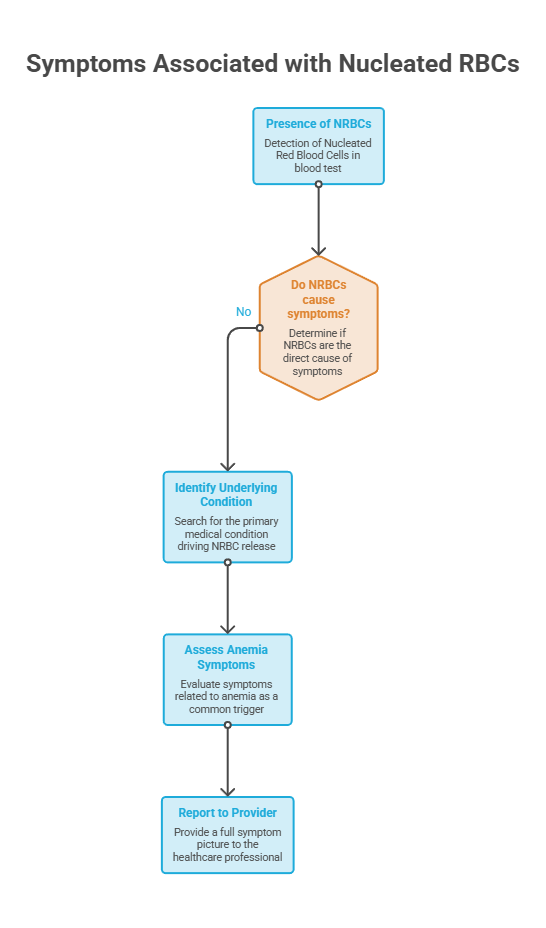
Because anemia is such a common trigger, the most frequent symptoms overlap with it. Knowing them helps you give your provider a fuller picture at your visit.
Anemia and Low-Oxygen Symptoms
Fatigue, weakness, pale skin, shortness of breath, dizziness, and a rapid heartbeat are classic signs that your blood isn’t carrying enough oxygen. These often accompany the anemias that raise NRBCs.
When low oxygen comes from a lung or heart condition, you may also notice breathlessness on exertion or a bluish tint to the lips or fingertips, which always warrants prompt attention.
Red-Flag Symptoms to Take Seriously
Some symptoms alongside NRBCs point to a more urgent problem. High fever, drenching night sweats, easy bruising or bleeding, bone pain, or unexplained weight loss all deserve prompt evaluation.
Confusion, severe breathlessness, or signs of serious infection paired with NRBCs are reasons to seek care quickly. Patients commonly ask us which symptoms can’t wait, and these sit at the top of the list.
What to Do About Nucleated RBCs in Your Results
A nucleated RBC finding calls for follow-up, not alarm. What matters is pairing the result with your symptoms, your history, and the rest of your CBC.
Use the table below as a quick guide to what different situations may mean and the sensible next step for each.
| Scenario | What It May Mean | Recommended Next Step |
| A single NRBC noted, you feel well | Often minor or transient | Discuss with your provider; likely a repeat CBC |
| Mild NRBCs with known anemia | Marrow responding to the anemia | Treat the anemia; recheck as advised |
| NRBCs plus abnormal white cells | Possible marrow infiltration | Prompt hematology evaluation and smear review |
| NRBCs with severe symptoms | Possible serious underlying illness | Seek prompt medical care |
| Newborn with NRBCs | Usually normal at birth | Routine monitoring per the pediatric team |
Questions to Ask Your Provider
Walking in prepared turns a worrying report into a productive visit. Ask what your exact NRBC value was, in both reporting formats if available, and how it compares to any earlier test.
It also helps to ask whether the rest of your CBC, like hemoglobin and the white cell differential, lines up with the finding, and whether you need a peripheral smear or further testing.
When It’s Urgent vs Routine
Many NRBC findings are followed up at a routine pace, especially a low-level result in someone who feels well. A known, treated anemia explaining the cells is reassuring context.
The picture changes with severe symptoms or worrying company on the smear. Immature white cells, fragmented red cells, or symptoms like high fever, breathlessness, or confusion alongside NRBCs deserve prompt medical attention.
Tracking NRBCs Over Time
For some people, a single NRBC result matters less than the trend across several tests. If you’re managing a chronic condition, your provider may recheck a CBC periodically to watch whether the count rises, falls, or clears.
A falling NRBC count after treatment is reassuring, while a rising one prompts a closer look. Patients we serve with treated anemia often repeat a CBC weeks later to confirm the cells have cleared.
Can Nucleated RBCs Return to Normal?
Whether NRBCs clear depends entirely on what’s driving them, which is one of the more reassuring parts of this topic for patients. Some triggers resolve and the cells vanish; others are chronic conditions managed over time.
Knowing which category your finding falls into helps set realistic expectations before you even start treatment.
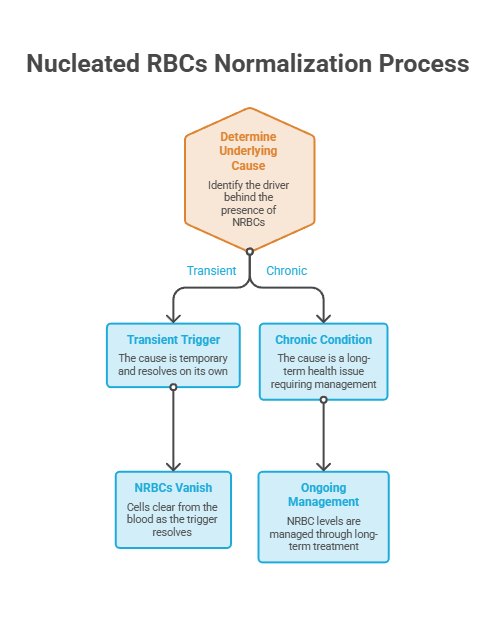
Reversible Triggers
When NRBCs reflect a temporary stress, treating that stress usually clears them. Correcting a treatable anemia, resolving an infection, or recovering from acute blood loss often returns the count to zero.
Patients we serve often see NRBCs clear from a follow-up CBC once the underlying trigger is treated. Because red blood cells live only about 120 days and turn over steadily, a repeat test a few months after the cause is addressed can look very different from the first.
Chronic or Serious Causes
When the cause is a lasting condition, NRBCs may persist or come and go. Sickle cell disease, thalassemia, chronic lung disease, and marrow disorders fall into this group.
Treatment still matters enormously. The American Society of Hematology notes that while there’s no universal cure for sickle cell disease, treatment helps people manage pain, prevent complications, and limit organ damage, and the same principle of managing the root cause applies broadly.
How NRBCs Fit Into the Bigger Blood Picture
NRBCs rarely tell their story alone. Read alongside the rest of your CBC, they become far more informative than a single line suggests.
A provider weighs them against your hemoglobin, your red cell indices, and your white cell differential to build a complete picture. That habit of reading the whole report is what separates a useful interpretation from a guess.
Pairing NRBCs With Hemoglobin and Hematocrit
If NRBCs appear with a low hemoglobin and hematocrit, the marrow is likely responding to anemia. If they appear with otherwise normal red cell numbers, the cause may lie elsewhere, such as marrow stress or infiltration.
This is why a standalone NRBC value is rarely acted on by itself. Patients booking a CBC through HealthCareOnTime are encouraged to review the full panel with their provider rather than fixating on one flagged cell type.
Pairing NRBCs With the White Cell Differential
The white cells keep important company. When NRBCs appear with immature white cells, that leukoerythroblastic pattern shifts attention toward the marrow itself.
When NRBCs appear with signs of infection in the white cell count, severe infection or sepsis moves up the list. The combination, not the NRBC alone, points the way.
Nucleated RBCs vs Reticulocytes: What’s the Difference?
People often confuse nucleated RBCs with reticulocytes, since both are young red blood cells. The difference comes down to maturity and what counts as normal.
A reticulocyte is one step further along: it has already shed its nucleus but still carries traces of RNA. A small number of reticulocytes circulate normally in healthy adults, because they’re nearly mature.
A nucleated red blood cell is younger and still has its nucleus, which is why it shouldn’t appear in adult blood at all. Both can rise when the marrow is replacing red cells quickly, so a provider may look at them together.
Our medical reviewers note that a high reticulocyte count signals active red cell production, while the appearance of NRBCs signals that production is intense enough, or the marrow disrupted enough, to push even less mature cells into circulation.
The Bottom Line on Nucleated RBCs
Nucleated red blood cells are immature cells that don’t belong in adult circulation, so finding them is a meaningful signal worth understanding. In newborns they’re expected, but in adults they point to bone marrow stress or an underlying condition.
The reassuring part is that many causes, especially treatable anemias and resolved infections, clear once addressed, and the cells follow. A high count in a seriously ill patient is a different matter that calls for close attention. Either way, the right move is the same: review the result with your provider, in the context of your full CBC, and let the cause guide what comes next.
Frequently Asked Questions
What does it mean to have nucleated RBCs in a blood test?
It means immature red blood cells, which still carry a nucleus, have entered your bloodstream. In adults this is abnormal and usually signals that the bone marrow is under stress or working hard, often from anemia, low oxygen, infection, or a marrow disorder. It always warrants follow-up to find the cause.
Is it normal to have nucleated red blood cells?
In healthy adults, no. The normal NRBC count is zero, because mature red cells shed their nucleus before entering circulation. Newborns are the exception and normally have some NRBCs that clear within the first weeks of life. Any adult finding should be interpreted by a provider.
What causes nucleated RBCs to appear?
Common causes include severe anemia and hemolysis (such as sickle cell disease or thalassemia), low oxygen from lung or heart disease, severe infection or sepsis, and bone marrow disorders like leukemia or myelofibrosis. In each case, the marrow is either replacing red cells rapidly or being disrupted by disease.
What is a normal NRBC level?
For adults, the normal level is 0 nucleated RBCs per 100 white blood cells. An ideal result is generally 0.3 per 100 WBC or less. Because the baseline is zero, there’s no meaningful “low” count in adults, so the focus is on why any are present.
Are nucleated RBCs a sign of cancer?
They can be, but they are not specific to cancer. NRBCs appear in many conditions, most commonly anemia, low oxygen, and infection. When they show up alongside immature white blood cells (a leukoerythroblastic picture), that pattern raises more concern for a marrow disorder and prompts further testing.
Are nucleated red blood cells normal in newborns?
Yes. A newborn’s blood normally contains some NRBCs at birth, reflecting the rapid red cell production of fetal life. These usually clear within the first few weeks. A higher-than-expected level can suggest stress before or during birth and is evaluated by the pediatric team.
What does a high NRBC count mean?
A higher count generally reflects greater bone marrow stress or demand. In critically ill patients, higher NRBC levels are linked to more severe illness and worse outcomes. In an outpatient setting, a high count still points to a significant underlying cause that needs prompt evaluation and likely further testing.
Should I worry about nucleated RBCs in my blood?
A finding deserves attention but not panic. The cause and your overall clinical picture determine its seriousness. A single NRBC in someone who feels well is very different from a high count with severe symptoms. Discuss the result with your provider, who can interpret it in context.
How are nucleated RBCs measured?
They’re counted as part of a CBC with differential, using an automated hematology analyzer, with a stained blood smear examined under a microscope for confirmation. Results are reported either as NRBCs per 100 white blood cells or as an absolute count per microliter of blood.
Can nucleated RBCs go back to normal?
Often, yes. When the trigger is temporary, such as a treatable anemia, a resolved infection, or recovery from blood loss, NRBCs usually clear and the count returns to zero. Chronic conditions may cause them to persist, though treating the underlying cause remains the goal.
What is normoblastemia?
Normoblastemia is the medical term for the presence of nucleated red blood cells (normoblasts) in the circulating blood. Since these immature cells normally stay in the bone marrow, normoblastemia signals that the blood-marrow barrier has been disrupted or that red cell production has surged.
What is a leukoerythroblastic reaction?
It’s a blood smear pattern showing nucleated red blood cells together with immature white blood cells. This combination suggests the bone marrow is being infiltrated or severely stressed, as in myelofibrosis, leukemia, or cancer that has spread to the marrow, and it typically prompts urgent hematology evaluation.
Medical Disclaimer: This article is for general informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Nucleated red blood cells are a laboratory finding, not a diagnosis on their own. Always discuss your blood test results with a qualified healthcare provider, and seek prompt care for severe or worsening symptoms.
References
- Healthline: Nucleated Red Blood Cell (NRBC) Blood Test
- SelfDecode Labs: NRBC (Nucleated RBC) Blood Test
- HealthMatters.io: Nucleated RBC (NRBC)
- NRBCs as a Prognostic Marker in Septic Critically Ill Patients (2025)
- NRBCs as a Prognostic Marker in SARS-CoV-2 ARDS (2024)
- NRBCs as Predictors of Mortality in ARDS (2018)
- NRBCs as Predictors of Mortality in Cardiac ICU Patients
- American Society of Hematology: Sickle Cell Disease
- NHLBI: Sickle Cell Disease





