Most wrist pain gets blamed on a sprain, a long day at the keyboard, or simply sleeping on it wrong. But when that ache lingers for months and never quite explains itself, the cause can be something far less ordinary: a small wrist bone slowly losing its blood supply.
Table of Contents
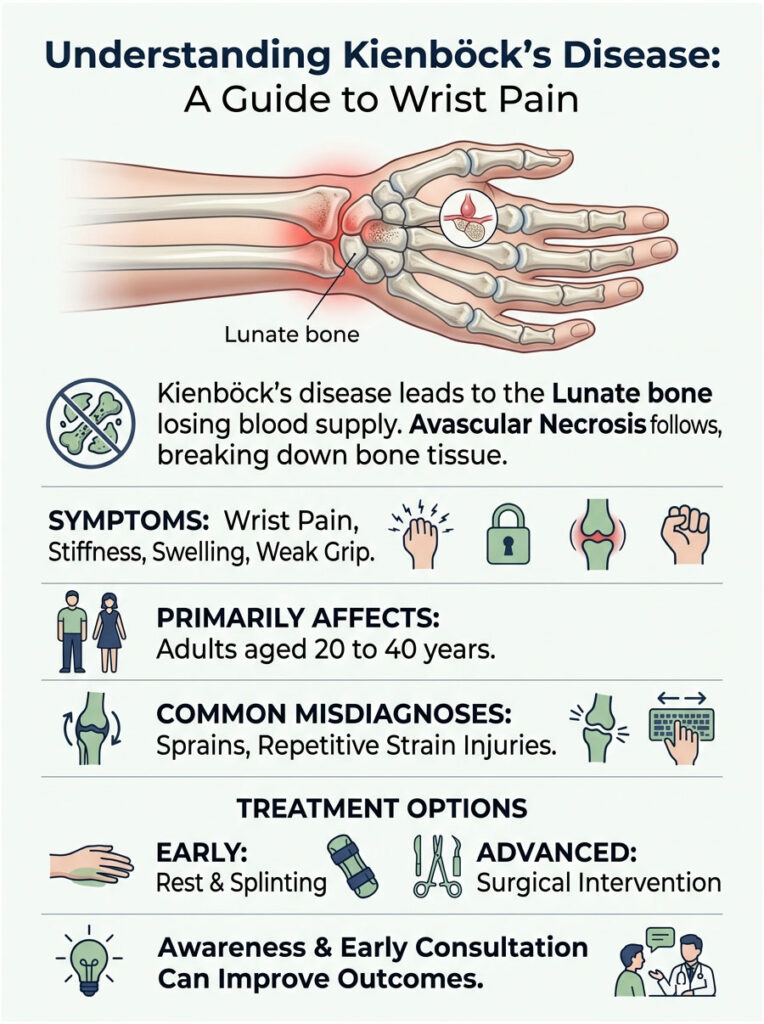
Quick Answer: Kienböck’s disease is a condition where the lunate, a small bone in the wrist, loses its blood supply and gradually breaks down, a process called avascular necrosis. It causes wrist pain, stiffness, swelling, and weak grip. It mainly affects adults aged 20 to 40. Treatment ranges from rest and splinting in early stages to surgery in advanced ones, guided by how far the disease has progressed.
At a Glance
- Kienböck’s disease is loss of blood supply to the lunate bone in the wrist.
- It typically affects one wrist, usually the dominant hand.
- Early symptoms closely mimic a simple wrist sprain.
- Men aged 20 to 40 are most commonly affected.
- MRI can detect it long before an X-ray shows damage.
- Treatment depends heavily on the stage at diagnosis.
What Kienböck’s Disease Actually Is
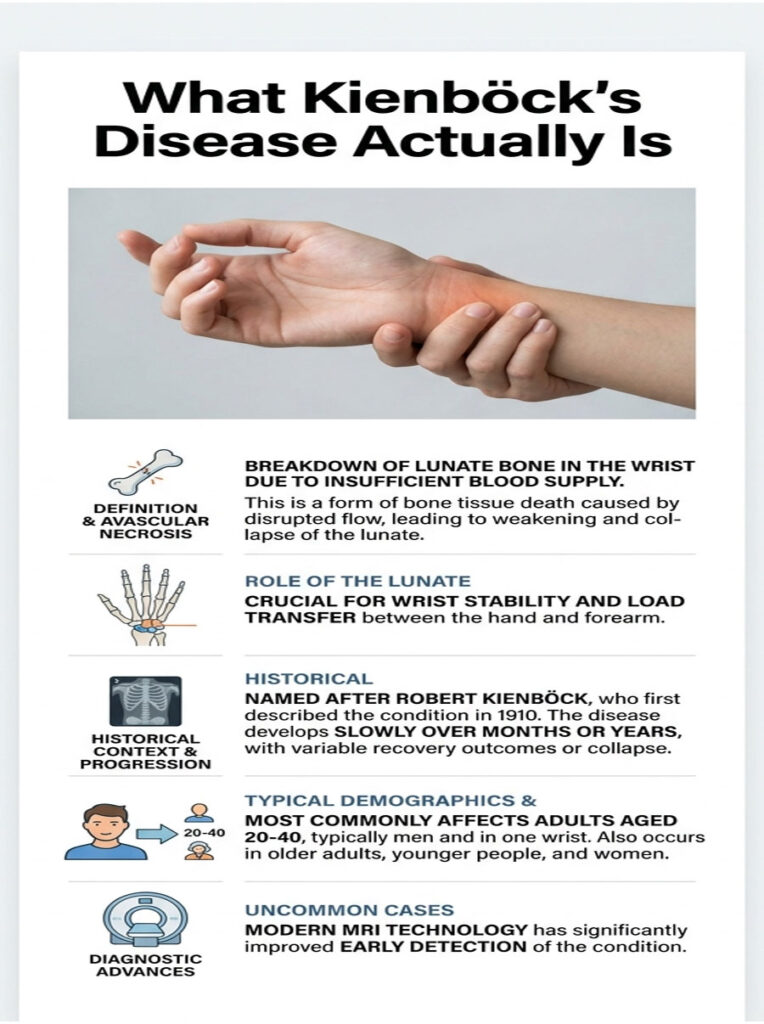
The name sounds intimidating, but the idea behind it is straightforward. Kienböck’s disease is the breakdown of one specific wrist bone after it stops getting enough blood.
The Lunate Bone and Why It Matters
Your wrist contains eight small carpal bones arranged in two rows. The lunate is a crescent-shaped bone sitting in the middle of the wrist, near where your forearm meets your hand.
It plays an outsized role for its size. The lunate helps transfer load from the hand to the forearm and contributes to smooth, stable wrist motion. When it weakens, the whole wrist suffers.
The lunate also sits at a mechanical crossroads. It articulates with the radius above and several carpal bones around it, so when the lunate fails, the forces it once shared get redistributed onto neighbors that were not built to carry them alone.
A Brief History of the Condition
The disease carries the name of Robert Kienböck, a Viennese radiologist who described osteonecrosis of the lunate in 1910. He used early X-ray technology to document the bone changes that still define the condition today.
More than a century later, the underlying cause still is not fully pinned down. What has improved dramatically is the ability to detect the disease early, thanks to modern MRI, which can reveal trouble long before an X-ray can.
What Goes Wrong: Avascular Necrosis Explained
Kienböck’s disease is a form of avascular necrosis, also called osteonecrosis. That term simply means bone tissue dying because it has lost its blood supply.
Living bone needs a steady flow of blood to stay healthy. When circulation to the lunate is interrupted, the bone starves, weakens, and over time can harden, collapse, and fragment. Our medical reviewers note that this is a slow process, often unfolding over months or years rather than days.
The process is not always one-directional. In some cases, blood supply partially recovers and the bone stabilizes; in others, it progresses to collapse. This variability is one of the things that makes the disease difficult to predict for any single person.
Who Develops Kienböck’s Disease
This condition has a recognizable profile. According to a clinical review published through the NIH, Kienböck’s disease most commonly affects adults between the ages of 20 and 40.
Men are affected roughly twice as often as women. It almost always involves just one wrist, typically the dominant hand. The condition is uncommon overall, which is part of why it is so frequently overlooked at first.
Despite that recognizable profile, the condition can appear outside the typical pattern. Older adults, younger people, and women all develop it, and a number of cases are found by chance on imaging done for an unrelated reason. A typical profile is a guide, not a rule.
Symptoms of Kienböck’s Disease
The symptoms of Kienböck’s disease are real but frustratingly vague in the beginning. That vagueness is exactly what makes the condition hard to catch early.
Early Symptoms That Mimic a Sprain
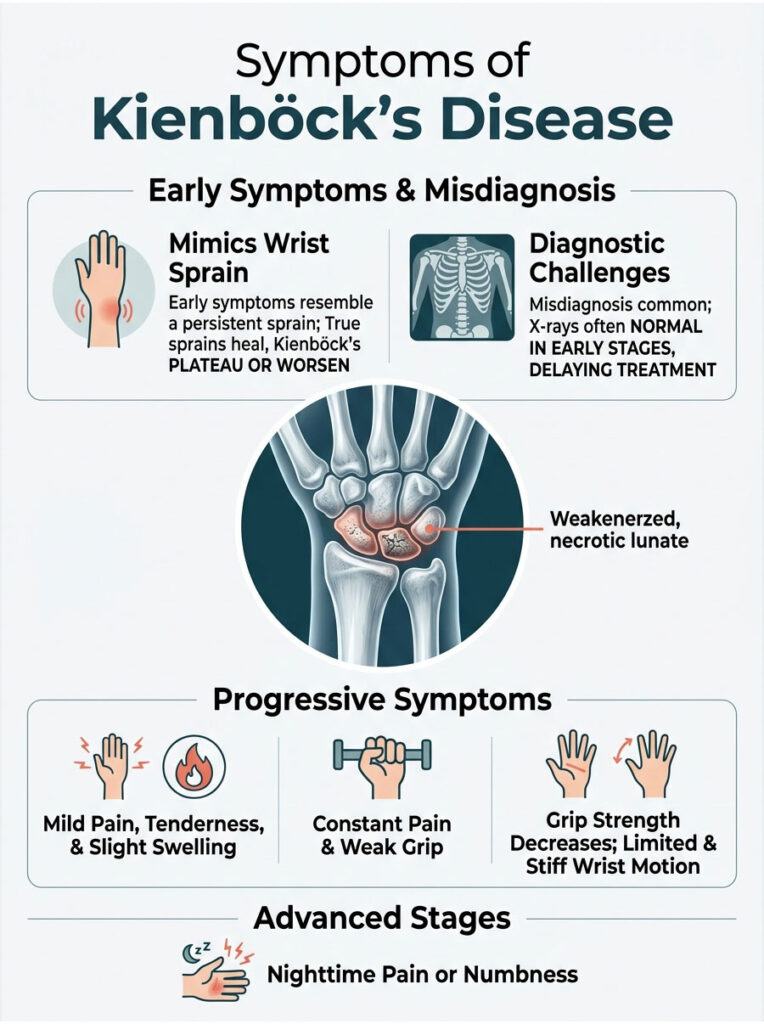
In the earliest stage, Kienböck’s disease often feels like a minor wrist sprain that simply won’t heal. There may be mild pain, some tenderness over the back of the wrist, and a bit of swelling.
Many people assume they tweaked the wrist and wait for it to settle. Patients booking diagnostic tests with us often describe months of background wrist pain they never thought serious enough to investigate.
One feature can hint that something more than a sprain is at work: time. A true sprain steadily improves over days to weeks, while Kienböck’s disease tends to plateau or slowly worsen. Pain that simply refuses to follow the normal healing curve deserves a closer look.
How Symptoms Progress
As the lunate weakens, symptoms intensify. Pain becomes more constant and can flare with gripping, lifting, or twisting the wrist.
Grip strength noticeably weakens, wrist motion becomes stiff and limited, and swelling can become more persistent. Some people are woken at night by a deep ache or the feeling that the hand has gone to sleep. In later stages, the wrist can feel mechanically unreliable.
It helps to picture the trajectory rather than a single moment. Early on, symptoms come and go and are easy to dismiss. As the bone weakens, the good days shorten and the painful ones stretch out, until the wrist limits everyday tasks rather than just demanding activities.
Why It’s So Often Missed
Kienböck’s disease is a master of disguise. Its early symptoms overlap with wrist sprains, tendinitis, and several forms of arthritis.
On top of that, a standard X-ray usually looks normal in the first stage, so an initial workup can come back falsely reassuring. In cases reviewed by our medical team, a delay of months between first symptoms and accurate diagnosis is common. The table below maps how the disease progresses through its recognized stages.
There is also a tendency to attribute wrist pain to whatever a person does most, blaming a keyboard, a sport, or a recent task. That instinct is reasonable but can anchor both patient and clinician on a wrong explanation, delaying the imaging that would reveal the real issue.
| Stage | Imaging Findings | Typical Symptoms | Common Treatment Approach |
| Stage 1 | X-ray normal; MRI shows lost blood supply | Mild pain, sprain-like ache | Rest, splinting, observation |
| Stage 2 | Lunate hardens, appears whiter on X-ray | Pain, soreness, swelling | Immobilization, joint leveling surgery |
| Stage 3 | Lunate collapses and begins to fragment | Growing pain, weak grip, stiffness | Joint leveling or salvage surgery |
| Stage 4 | Surrounding carpal bones degenerate | Significant pain, arthritis, limited motion | Salvage surgery, fusion, or carpectomy |
What Causes Kienböck’s Disease
Here is the honest truth that competitors often gloss over: the exact cause of Kienböck’s disease is still not fully understood. What experts have identified is a set of contributing factors.
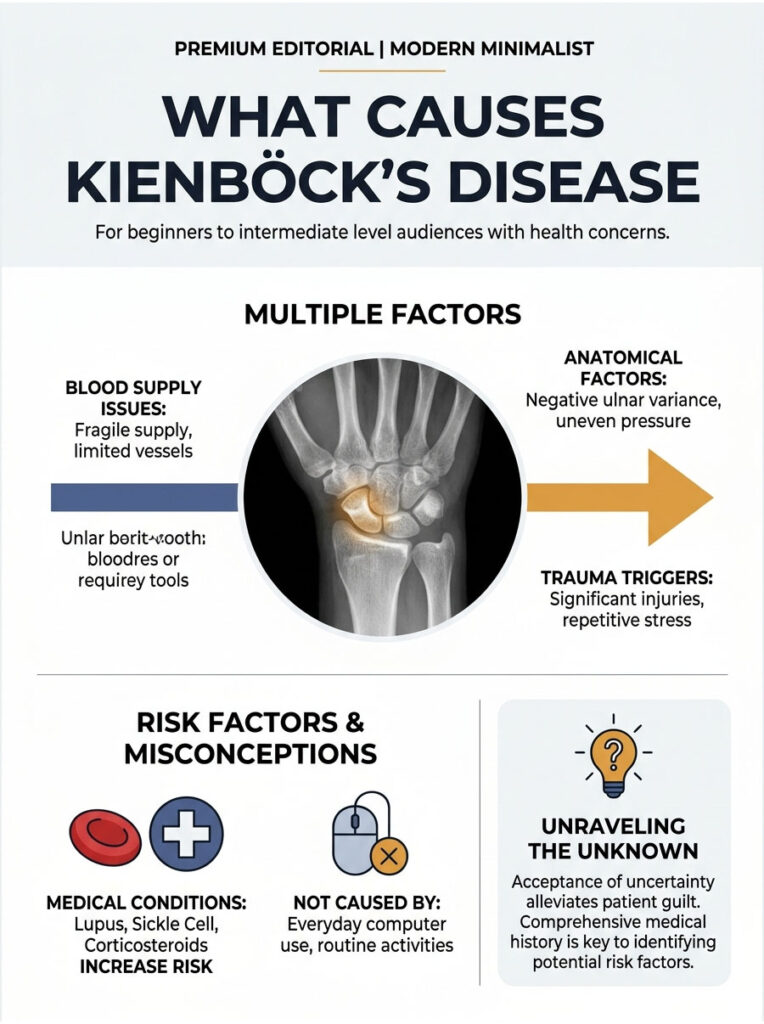
Understanding the cause matters for a practical reason. Patients often blame themselves, searching for the one thing they did wrong, whether a job, a sport, or an old injury. In most cases there is no such single thing, and accepting that the cause is genuinely uncertain can ease a good deal of unnecessary guilt and worry.
Blood Supply and Vascular Factors
At its core, the problem is circulation. The lunate’s blood supply can be relatively fragile, sometimes fed by only one or two small vessels.
Anything that disrupts that delicate supply, such as repeated small injuries or impaired blood drainage, can tip the bone toward necrosis. Some people are simply born with a more vulnerable blood supply pattern to the lunate.
Researchers describe the cause as multifactorial, meaning several factors likely combine rather than one acting alone. A person may have a borderline blood supply, an anatomical quirk, and a history of wrist stress, with no single one being enough on its own.
Ulnar Variance and Wrist Anatomy
Wrist anatomy plays a part. The two forearm bones, the radius and the ulna, normally meet the wrist at nearly the same level.
When the ulna sits shorter than the radius, a setup called negative ulnar variance, the lunate may take on uneven pressure. This anatomical pattern has long been associated with Kienböck’s disease, though research has not confirmed it as a definite cause, and many patients have normal anatomy.
Ulnar variance is measured on a wrist X-ray and is described as negative, neutral, or positive. While negative variance has drawn the most research attention, the disease occurs across all three patterns, a reminder that anatomy is only one piece of the puzzle.
Trauma, Repetitive Stress, and Medical Risk Factors
Injury is a recognized trigger. A single significant wrist trauma, or repeated microtrauma from jobs and activities that load the wrist hard, can contribute.
Certain medical conditions raise the risk too, including lupus, sickle cell disease, cerebral palsy, and long-term corticosteroid use. Our lab partners report that a thorough history often surfaces one or more of these threads, even when no single clear cause stands out.
It is worth being clear about what does not cause the disease. Everyday computer use, normal household activity, and ordinary exercise are not established causes. Worrying that routine life triggered the condition is common but generally unfounded.
How Kienböck’s Disease Is Diagnosed
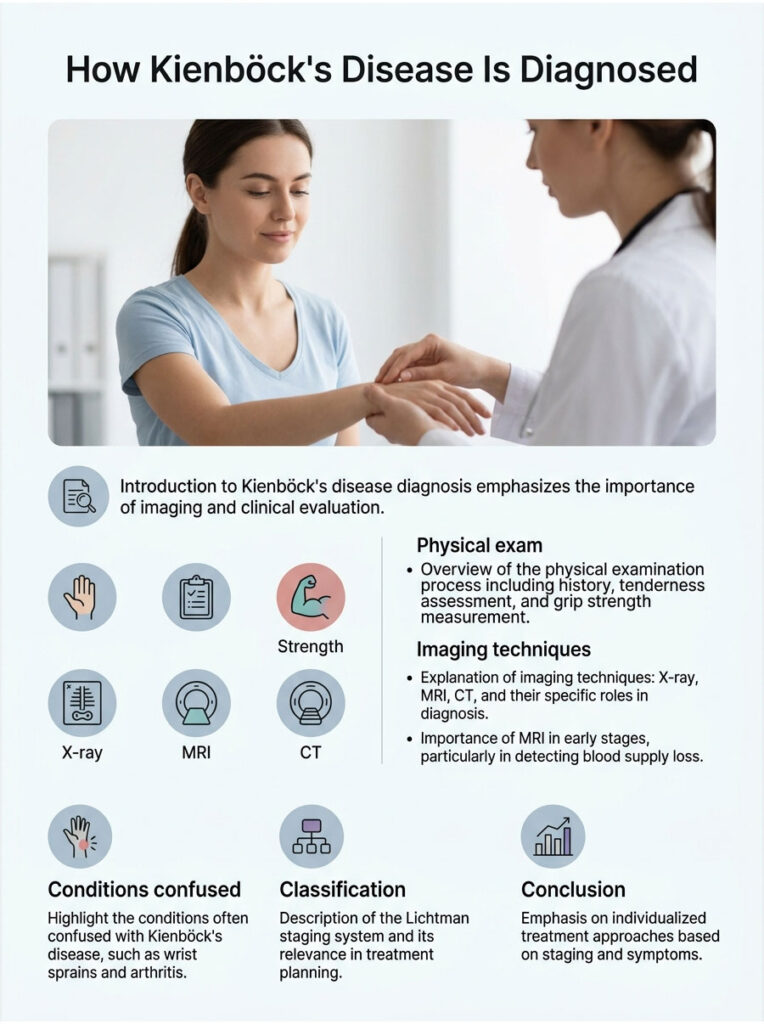
The symptoms point in too many directions to diagnose this condition by feel alone, so imaging and a careful clinical eye carry the weight. Getting the stage right matters, because it shapes every treatment decision that follows.
Physical Examination
The process starts with a conversation and a hands-on exam. A doctor will ask about the pain’s history, your work and activities, and any past wrist injuries.
They will check for tenderness over the lunate, assess swelling, measure grip strength, and test how far the wrist moves. These findings are suggestive but rarely conclusive on their own.
The exam also helps a clinician decide which imaging to order and how urgently. A wrist that is merely tender is approached differently from one that is visibly swollen, weak, and stiff, even before any scan is done.
Imaging: X-ray, MRI, and CT
Imaging is where the diagnosis is confirmed. An X-ray is usually the first test, and it can reveal hardening, collapse, or fragmentation of the lunate in later stages.
A CT scan gives a detailed look at bone structure and can map the number and size of bone fragments. Each imaging type answers a different question about the bone.
A bone scan is another tool a doctor may use, since it can highlight areas of unusual bone activity. The choice of imaging is not random; each test is ordered to answer a specific question raised by the exam.
X-rays remain valuable despite their early-stage blind spot. They are quick, widely available, and good at tracking change over time, which is why doctors often repeat them as a way to monitor whether the lunate is holding steady or progressing.
Conditions Often Confused With Kienböck’s Disease
Because wrist pain has many sources, several conditions can look like Kienböck’s disease at first. Wrist sprains, tendinitis, and ganglion cysts all produce overlapping discomfort, and various forms of arthritis can mimic it closely.
Ulnar-sided wrist impaction and certain rare bone lesions also enter the picture. This overlap is exactly why imaging, especially MRI, carries so much weight. A careful specialist works through these possibilities rather than settling on the first plausible label.
Why MRI Matters in Early Stages
Here is the detail that changes outcomes. In Stage 1, an X-ray typically looks completely normal, which is why early Kienböck’s disease is so often missed.
An MRI, by contrast, can detect the loss of blood supply to the lunate before any structural damage appears. When wrist pain persists despite a normal X-ray, an MRI is the test that can find the problem early, while treatment options are widest.
The Lichtman Staging System
Doctors classify Kienböck’s disease using the Lichtman staging system, which runs from Stage 1 to Stage 4. It is based on imaging findings and describes how far the bone breakdown has advanced.
Staging is useful but not perfect. The system describes the bone’s appearance, yet it does not always match how much pain or limitation a person feels. Two people at the same stage can have noticeably different symptoms, which is why treatment is tailored to the individual, not the label alone.
This staging is more than academic. According to NIH StatPearls, staging is essential for treatment planning, since the right approach for an early case differs sharply from that for a collapsed lunate. The data below puts the condition in context.
| Metric | Figure | Source |
| Most affected age range | 20 to 40 years | NIH (PMC) |
| Male-to-female ratio | About 2 to 1 | JBJS Open Access |
| Radiographic prevalence of incidental disease | About 7 per 100,000 patients | NIH (PMC) |
| Wrists typically involved | One, usually the dominant hand | PubMed |
| Staging system used | Lichtman, Stage 1 to 4 | NIH StatPearls |
Kienböck’s Disease Treatment Options
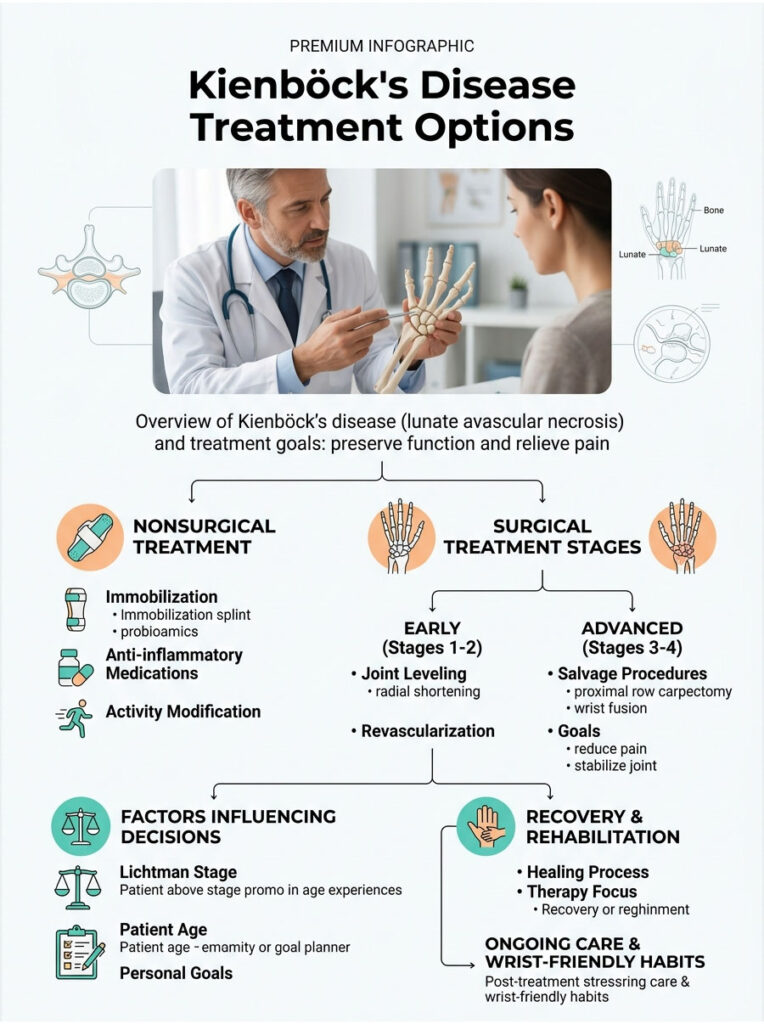
There is no single fix for Kienböck’s disease, and no treatment that fully reverses it. The goal is to relieve pain, preserve wrist function, and slow or halt the disease’s progression. The right approach depends almost entirely on the stage.
Nonsurgical Treatment
In the earliest stages, before the lunate has collapsed, nonsurgical care is often the first step. The aim is to take pressure off the bone and give it the best chance to recover.
This usually means immobilizing the wrist in a splint or cast for a period of weeks, sometimes months. Anti-inflammatory medications such as ibuprofen can manage pain and swelling. Our medical reviewers note that nonsurgical care can ease symptoms, though it does not reliably stop the disease from advancing.
Activity modification is part of nonsurgical care too. Reducing heavy gripping, repetitive loading, and high-impact use of the affected wrist takes strain off the lunate. A hand therapist can help identify which daily movements to adjust.
Nonsurgical care also serves as a useful trial. If symptoms settle with rest and splinting, that is encouraging; if they persist or worsen despite it, that information itself helps guide the decision toward surgical options.
Surgical Treatment by Stage
When the disease progresses or pain persists, surgery is considered. There are several procedures, and the choice depends on the stage and the patient.
No single procedure suits every patient, and surgery for Kienböck’s disease continues to be studied. Outcomes can be good, but because the disease itself has no cure, the realistic aim is durable pain relief and a functional wrist rather than a perfectly normal one.
Joint Leveling and Revascularization
For earlier stages, surgeons often aim to protect the lunate. Joint leveling procedures adjust the length of the radius or ulna to redistribute pressure away from the struggling bone.
Revascularization attempts to restore blood flow to the lunate, sometimes by transferring a small piece of vascularized bone. These approaches work best in Stages 1 and 2, before the lunate has fragmented.
These reconstructive procedures share a goal: change the mechanics or biology around the lunate so the bone has a fighting chance. Their success depends heavily on catching the disease before the bone has collapsed, which again points back to early diagnosis.
Salvage Procedures for Advanced Disease
When the lunate has collapsed or surrounding bones have degenerated, the focus shifts to salvaging wrist function. Options include proximal row carpectomy, which removes a row of carpal bones, and partial or full wrist fusion.
These procedures trade some range of motion for lasting pain relief and stability. They are reserved for advanced disease where preserving the lunate is no longer realistic.
Salvage does not mean failure. For a wrist that is already painful and stiff, a well-chosen salvage procedure can restore comfort and reliable function, which often matters more to daily life than preserving every last degree of motion.
How Treatment Decisions Are Made
Choosing a path is rarely a single obvious answer. A surgeon weighs the Lichtman stage, the patient’s age, pain level, hand dominance, job demands, and personal goals.
A young manual worker and an older person with light wrist demands may reasonably choose different routes for the same stage. Patients commonly ask us for the best surgery, and the honest answer is that the best option is the one matched to that specific wrist and life, decided together with a hand specialist.
Time itself is a factor in the decision. Because earlier stages carry more options, a diagnosis caught early often allows a calmer, less pressured choice, while advanced disease can narrow the path considerably.
Recovery and Rehabilitation
Recovery varies widely by procedure. Healing after surgery can take weeks to months, and most people work with a hand therapist afterward.
Therapy focuses on regaining motion, rebuilding grip strength, and learning wrist-friendly ways to handle daily tasks. The honest answer to how long it takes is that it depends on the surgery and the individual, often spanning several months.
Protecting the result matters as much as achieving it. After healing, many people benefit from ongoing wrist-friendly habits, periodic check-ins with their care team, and prompt attention if new symptoms appear. Recovery is less a finish line than a new baseline to maintain.
Living With Kienböck’s Disease and Long-Term Outlook
A Kienböck’s diagnosis raises understandable worry about the future. The realistic picture is mixed, but far from hopeless.
Prognosis and What to Expect
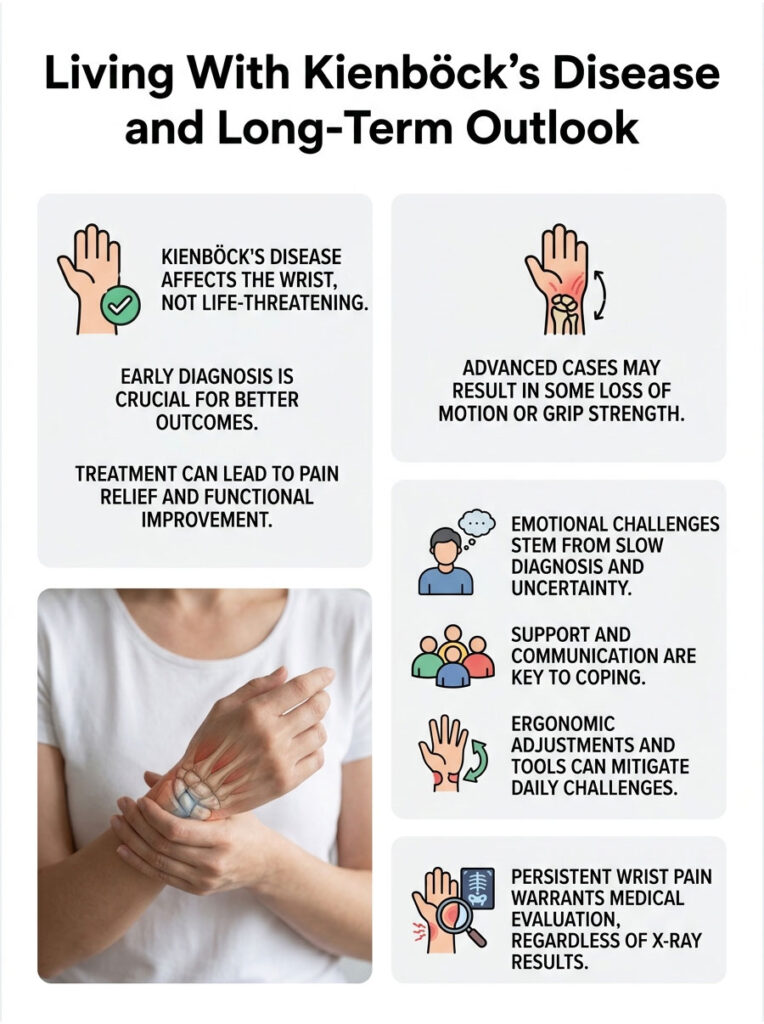
Kienböck’s disease has no complete cure, and outcomes depend largely on how early it is caught. Treated early, many people achieve good, lasting pain relief and functional wrists.
In advanced cases, some loss of motion or grip strength may remain even after successful surgery. The disease is not life-threatening, and it affects the wrist alone. Across patients we serve, early diagnosis is consistently the strongest predictor of a good outcome.
One uncertainty is worth naming honestly. The natural history of Kienböck’s disease is incompletely understood, and not every case marches predictably toward collapse. Some appear to stabilize, which is part of why monitoring is a legitimate option for certain patients.
It also helps to keep the condition in proportion. Kienböck’s disease is a wrist problem, not a systemic illness. It does not spread to other joints or organs, and with the right plan most people continue to work, exercise, and live full lives.
Coping With a Slow, Uncertain Diagnosis
Kienböck’s disease can be emotionally taxing in a quiet way. It often takes months to diagnose, has an unclear cause, and unfolds slowly, which can leave people feeling stuck in limbo.
That experience is normal and worth naming. Connecting with a hand specialist who can explain the stage clearly, set realistic expectations, and lay out a plan tends to replace uncertainty with a sense of direction.
Support helps carry the uncertainty. Talking with others who have a wrist condition, leaning on family for tasks during flare-ups, and being patient with yourself are all reasonable. A diagnosis that unfolds slowly asks for steady coping, not a single brave decision.
Daily Life, Work, and Activity
For many people, Kienböck’s disease affects work and hobbies that load the wrist, such as manual labor, sports, or heavy lifting. Modifications often help.
A hand therapist can suggest ergonomic adjustments, supportive splinting for certain tasks, and technique changes that reduce strain. Whether the condition counts as a disability depends on its severity, the demands of a person’s job, and individual circumstances.
Small tools and habits make a real difference. Built-up grips on utensils and pens, jar openers, two-handed lifting, and voice-to-text for heavy typing all reduce strain. Occupational therapists are skilled at matching these adjustments to a person’s specific routine.
Open conversations at work can help too. Many employers will accommodate temporary changes, such as lighter duties or assistive equipment, once they understand the situation. Framing it as a practical, time-limited need usually goes further than waiting until the wrist forces the issue.
When to See a Doctor
Wrist pain that lasts more than a few weeks, especially if it does not improve with rest, deserves a medical evaluation. This is doubly true if grip strength is fading or motion is becoming limited.
A normal X-ray does not rule out Kienböck’s disease, so persistent, unexplained wrist pain is worth pursuing further. The decision table below offers quick guidance.
There is no downside to having persistent wrist pain checked. If it turns out to be a minor strain, that is good news, and if it is something more, early diagnosis is the single biggest advantage a patient can have with this condition.
| Scenario | What It May Mean | Recommended Action |
| Wrist pain over 4 weeks, not improving | Possible early Kienbock’s or other issue | See a doctor for evaluation |
| Persistent pain but normal X-ray | Early-stage disease may be hidden | Ask whether an MRI is appropriate |
| Worsening grip strength and stiffness | Possible disease progression | Seek prompt orthopedic assessment |
| Confirmed early-stage diagnosis | Treatment options are widest now | Discuss nonsurgical and surgical paths |
| Advanced pain with limited motion | Likely later-stage disease | Consult a hand surgeon |
| Sudden severe wrist pain after injury | Fracture or acute injury possible | Seek same-day medical care |
Questions to Ask Your Doctor
A Kienböck’s diagnosis comes with a lot to absorb. Walking into an appointment with a short list of questions helps turn a confusing visit into a clear plan.
Useful questions include: What Lichtman stage is my disease, and what does that mean? Is my condition likely to progress, and how fast? Which treatment options fit my stage, age, and activities?
It is also fair to ask: What happens if I choose to wait and monitor? What can I expect for pain relief and wrist function with each option? And how will we track whether the chosen approach is working?
Bringing a family member or friend, and taking notes, makes it easier to remember the answers later. Patients we work with consistently find that a prepared visit leads to better decisions and less second-guessing afterward.
Frequently Asked Questions
What is Kienböck’s disease in simple terms?
Kienböck’s disease is a condition where a small wrist bone called the lunate loses its blood supply and slowly breaks down. Without enough blood, the bone weakens, can collapse, and causes wrist pain, stiffness, and reduced grip strength over months or years.
What are the first signs of Kienböck’s disease?
The earliest signs are subtle and feel like a wrist sprain that won’t heal. Expect mild pain, tenderness over the back of the wrist, slight swelling, and sometimes a bit of stiffness. Because these symptoms are vague, the condition is often overlooked at first.
Is Kienböck’s disease curable?
There is no complete cure for Kienböck’s disease, and no treatment fully reverses it. However, treatment can relieve pain, preserve wrist function, and slow progression. Outcomes are best when the disease is caught early, before the lunate bone collapses or fragments.
What causes Kienböck’s disease?
The exact cause is unknown. It develops when the lunate loses its blood supply, and contributing factors include a naturally fragile blood supply, wrist trauma or repetitive stress, and anatomical patterns like negative ulnar variance. Certain medical conditions and long-term steroid use also raise the risk.
How is Kienböck’s disease diagnosed?
Diagnosis combines a physical exam with imaging. X-rays show bone changes in later stages but often look normal early on. An MRI can detect lost blood supply to the lunate before structural damage appears, and a CT scan maps bone fragments in advanced disease.
Can Kienböck’s disease be treated without surgery?
In early stages, yes. Nonsurgical treatment includes immobilizing the wrist with a splint or cast and using anti-inflammatory medication for pain. This can ease symptoms, but it does not reliably stop the disease from progressing, so close monitoring is important.
What happens if Kienböck’s disease is left untreated?
Untreated, the disease tends to progress. The lunate can harden, collapse, and fragment, which shifts other wrist bones out of position and can lead to arthritis across the wrist. This typically means worsening pain, weaker grip, and increasingly limited motion.
Who is most likely to get Kienböck’s disease?
Kienböck’s disease most often affects adults between 20 and 40 years old, and men are affected about twice as often as women. It usually involves the dominant wrist. People with certain medical conditions or a history of wrist trauma may be at higher risk.
Is Kienböck’s disease a disability?
It depends on severity and circumstances. Mild cases may cause little lasting limitation, while advanced disease can significantly affect grip and wrist motion. Whether it qualifies as a disability depends on the impact on a person’s specific job and daily function.
How long does recovery from Kienböck’s surgery take?
Recovery varies by procedure and patient. Healing generally takes several weeks to a few months, often followed by hand therapy to rebuild motion and grip strength. Your surgeon can give a timeline based on the specific operation performed.
Can Kienböck’s disease come back after treatment?
Treatment aims to relieve pain and preserve function, but because there is no full cure, symptoms can sometimes persist or progress, especially if the disease was advanced. Ongoing follow-up helps a care team monitor the wrist and adjust the plan as needed.
Does Kienböck’s disease affect both wrists?
It almost always affects just one wrist, typically the dominant hand. Cases involving both wrists are rare. If both wrists have similar symptoms, a doctor may look for other conditions that can mimic Kienböck’s disease.
Medical Disclaimer: This article is for general educational purposes only and does not replace professional medical advice, diagnosis, or treatment. HealthCareOnTime.com does not diagnose conditions or recommend specific treatments. Kienböck’s disease requires evaluation by a qualified healthcare provider, ideally a hand or orthopedic specialist, who can stage the condition and recommend an appropriate plan.
References
- NIH (PMC) – Kienbock’s Disease: Case Report and Review of the Literature
- NIH StatPearls – Kienbock Disease
- NIH (PMC) – The Radiological Prevalence of Incidental Kienbock Disease
- Cleveland Clinic – Kienbock’s Disease
- NORD – Kienbock Disease
- JBJS Open Access – Clinical and Radiographic Outcomes in Kienbock Disease