

Your blood test comes back, you scan it, and there it is: a little “L” next to your red blood cell count. Your stomach drops. Here’s what almost no one tells you first. That low reading is usually your body working exactly as designed.
Table of Contents
Roughly 1 in 4 US pregnancies meets the medical definition of anemia, yet a falling RBC count is the norm in pregnancy, not the alarm. The real skill is knowing where the expected dip ends and a genuine problem starts.
Quick answer: Red blood cell counts normally fall during pregnancy because plasma (the liquid part of blood) expands faster than red cell mass, diluting the blood. This is called physiologic anemia. Typical RBC ranges run about 3.42 to 4.55 million cells per microliter in the first trimester and dip lowest in the second. A count modestly below your pre-pregnancy number is usually fine. Counts well under range, or symptoms like dizziness and breathlessness, deserve a call to your OB.
At a glance
- Your RBC count is expected to drop during pregnancy; the lowest point is usually the second trimester.
- The cause is hemodilution: plasma volume rises 40% to 50%, red cell mass only 20% to 30%.
- True anemia (most often iron deficiency) affects roughly 25% of US pregnancies and needs treatment.
- Iron needs jump to 27 mg a day, well above what the average American diet provides.
- Low RBC matters when it dips far below range or comes with real symptoms.
- High RBC is rarer but worth flagging, often a sign of dehydration.
What Red Blood Cells Do and Why Pregnancy Changes Them
Red blood cells are your body’s oxygen delivery trucks. Each is packed with hemoglobin, the iron-rich protein that grabs oxygen in your lungs and hands it off to every tissue, including the placenta feeding your baby.
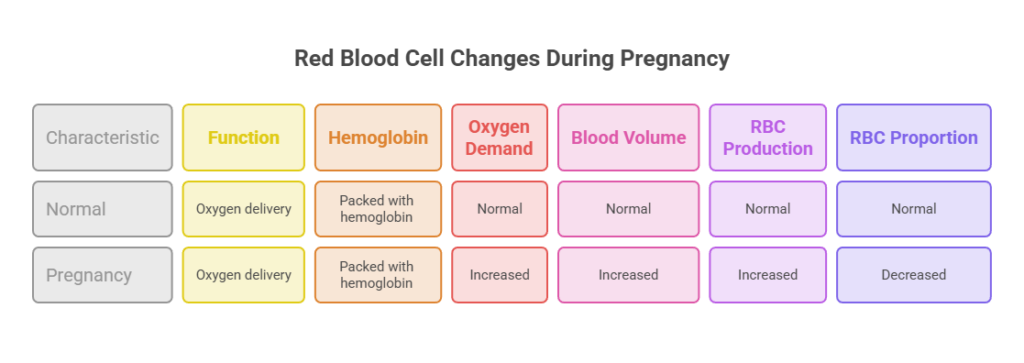
Pregnancy cranks up the demand for oxygen, so your body makes more blood. The twist is that it doesn’t add the parts in equal measure, and that imbalance explains your whole shifting RBC picture.
RBCs, hemoglobin, and oxygen for two
A blood test reports your RBC count as the number of red cells in a set volume of blood. Sitting right beside it are hemoglobin and hematocrit, two numbers that rise and fall with your RBC count and tell a matching story about oxygen-carrying power.
Those three values headline every pregnancy blood panel. In CBC results reviewed by our medical team, they’re the first numbers an OB checks to confirm you’re building enough red cells for both you and your baby.
Plasma volume versus red cell mass
Total blood volume climbs about 50% during pregnancy. The catch is that watery plasma expands by roughly 40% to 50%, while red cell mass grows by only 20% to 30%, per clinical data summarized in Williams Obstetrics reference ranges.
Picture stirring one scoop of cocoa into a steadily bigger cup of water. The cocoa never leaves, but every sip tastes more diluted. Your red cells are the cocoa; your blood simply gets watered down.
That dilution is why your RBC count, hemoglobin, and hematocrit all read below your pre-pregnancy baseline. Clinicians call it physiologic anemia of pregnancy. The word “physiologic” is the reassuring part, since it means normal, not diseased.
Dilution peaks in the second trimester, when plasma expansion is greatest. Our reviewers note that this mild dip is one of the most common “abnormal” flags expecting patients ask us to explain, and it usually needs nothing more than reassurance and routine iron.
Normal RBC Levels by Trimester (US Reference Chart)
So what actually counts as normal? “Normal” moves as your pregnancy advances, which is exactly why one fixed number won’t do. The chart below uses widely cited US clinical reference ranges so you can watch the targets shift.
| Stage | RBC (million/µL) | Hemoglobin (g/dL) | Hematocrit (%) |
| Non-pregnant adult woman | 4.00 to 5.20 | 12.0 to 15.8 | 35.4 to 44.4 |
| First trimester | 3.42 to 4.55 | 11.6 to 13.9 | 31 to 41 |
| Second trimester | 2.81 to 4.49 | 9.7 to 14.8 | 30 to 39 |
| Third trimester | 2.71 to 4.43 | 9.5 to 15.0 | 28 to 40 |
| Anemia cutoff (flag for follow-up) | Below trimester range | Under 11 (T1), 10.5 (T2), 11 (T3) | Under 33 (T1), 32 (T2), 33 (T3) |
Ranges adapted from Abbassi-Ghanavati et al. and Williams Obstetrics; anemia cutoffs reflect ACOG and CDC guidance.
Hemoglobin and hematocrit, the numbers beside RBC
Your RBC count rarely travels alone on a report. Hemoglobin tells you how much oxygen-carrying protein your blood holds, and hematocrit is the share of your blood made up of red cells, so a hematocrit of 33% means red cells fill about a third of the sample.
All three slide downward together during pregnancy for the same dilution reason. Because hemoglobin maps most directly to symptoms and oxygen delivery, it’s the value your provider leans on hardest when deciding whether you’re anemic.
Why the second trimester reads lowest
See how the bottom of each range slides down through the second trimester, then nudges back up in the third? That dip isn’t a warning sign by itself; it’s the predictable floor of hemodilution.
By late pregnancy, red cell production catches up somewhat, so many women watch their numbers tick upward before delivery. Across the pregnant patients we serve, a second-trimester low that recovers in the third is a textbook normal pattern.
When a lab flags “low” that isn’t really low
Lab software usually compares your result against non-pregnant ranges, so a healthy pregnancy value can earn an automatic “L.” That flag scares a lot of people for no reason.
The number that truly defines anemia in pregnancy is hemoglobin, set per trimester: under 11 g/dL in the first, under 10.5 in the second, under 11 in the third, per ACOG criteria. If your value falls inside the pregnancy range, a generic “low” tag usually isn’t worth worrying over. Your OB reads it against the right yardstick.
Why Your RBC Count Drops (and When It’s Not Just Dilution)
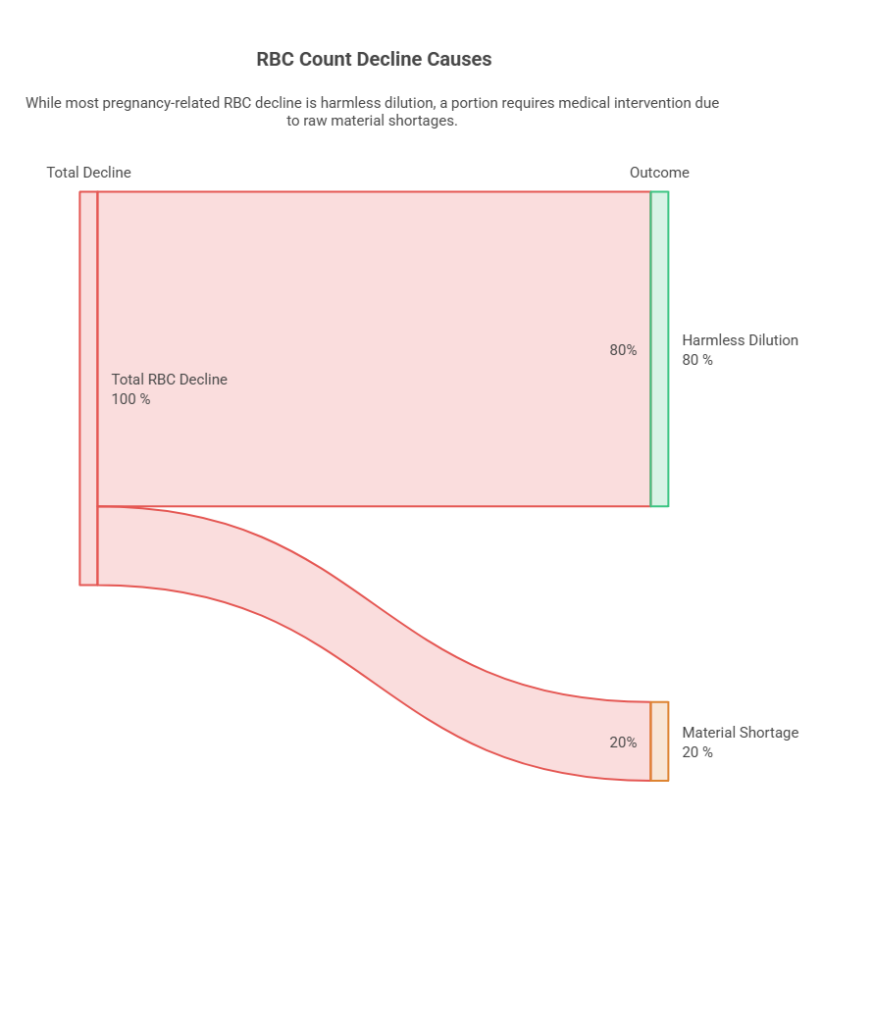
Most of the decline you’ll see is harmless dilution. Not all of it, though. Sometimes a low count signals a real shortage of the raw materials your body needs to build red cells, and those cases call for treatment.
Physiologic (dilutional) anemia, the normal kind
This is the default and the most common explanation. Your red cell mass is genuinely growing; it just can’t match the surge in plasma. A telling clue is that your MCV (a measure of red cell size) stays normal, since the existing cells are perfectly healthy, just outnumbered.
Iron-deficiency anemia, the most common true cause
When the drop runs past simple dilution, iron is usually behind it. Iron-deficiency anemia makes up about 75% of all anemia in pregnancy, according to clinical reviews cited by Medscape.
The math is simple and unforgiving. A single pregnancy demands roughly 1,000 mg of extra iron to build the baby’s blood supply, expand your own, and cover delivery losses. Plenty of women start pregnancy without enough banked iron to pay that bill.
Folate and B12 deficiency
Iron isn’t the only building block. Folate and vitamin B12 are both needed to make healthy red cells, and a shortfall in either can trigger anemia, often with enlarged cells (a high MCV). That’s one reason prenatal vitamins pair folic acid with iron.
Less common causes worth ruling out
Inherited conditions like thalassemia, sickle cell disease, and G6PD deficiency can lower counts or shorten red cell lifespan, and acute blood loss is another cause. A markedly low RBC count, especially early on, deserves a workup rather than being written off as “just pregnancy.” If you want to decode the individual cell measurements behind your count, our related guides on RDW and red cell morphology break those numbers down.
Telling dilution from a true deficiency
How does your provider know which kind of low count you have? The red cell indices do a lot of the work. A normal MCV alongside mildly low numbers points to simple dilution, while small, pale cells (a low MCV and MCH) flag iron deficiency.
When the picture is murky, a ferritin test measures your iron stores directly, and a reticulocyte count shows whether your marrow is pumping out fresh cells. In panels we help patients interpret, ferritin is often the single most useful add-on when a count looks borderline.
Low RBC in Pregnancy: Symptoms and Risks to Watch
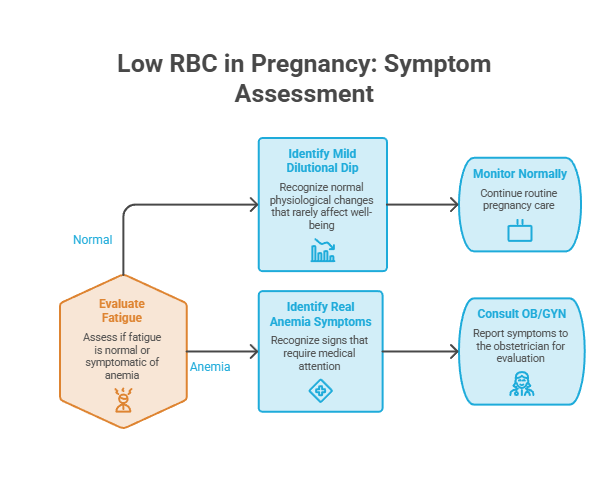
A mild dilutional dip rarely changes how you feel. Real anemia does, and learning its symptoms helps you separate ordinary “pregnancy tired” from something your OB should hear about.
Everyday symptoms
Mild anemia tends to whisper before it shouts. Watch for unusual fatigue, weakness, pale skin, lightheadedness, headaches, and breathlessness after light activity. Cold hands and feet and brittle nails can join the list.
The tricky part is that pregnancy itself brings plenty of fatigue. A little tiredness alone isn’t proof of anemia; the cluster and severity of symptoms are what count.
When symptoms cross into red-flag territory
Some signs deserve a same-day call rather than a wait-and-see approach. A racing or pounding heart, breathlessness at rest, chest pain, fainting, or dizziness bad enough to derail your day all point toward symptomatic anemia.
Pica, the urge to chew ice or non-food items like clay or starch, is a classic and underrecognized sign of iron deficiency. Patients booking tests with us often mention an ice habit without realizing it’s a clue worth reporting.
Risks to mother and baby
Untreated anemia isn’t just uncomfortable. Iron-deficiency anemia is linked to higher risks of preterm birth, low birth weight, and perinatal complications, and it leaves mothers more vulnerable if heavy bleeding strikes at delivery. That’s the practical reason screening and treatment matter.
The encouraging flip side: caught early, most pregnancy anemia responds well to iron. The table below maps common scenarios to sensible next steps.
| Your result or situation | What it likely means | Recommended action |
| RBC slightly below pre-pregnancy, no symptoms | Physiologic (dilutional) anemia | Keep taking prenatal iron; routine monitoring |
| Hemoglobin just under the trimester cutoff | Mild anemia, often iron deficiency | Ask about iron dosing and a ferritin check |
| Low RBC with low MCV (small cells) | Likely iron-deficiency anemia | Start iron as advised; recheck in 2 to 4 weeks |
| Low RBC, normal MCV, high RDW | Possible mixed deficiency | Request iron, B12, and folate testing |
| Dizziness, breathlessness, racing heart | Symptomatic anemia | Call your OB promptly |
| High RBC early with frequent vomiting | Likely dehydration | Rehydrate; report persistent values to your OB |
Call your OB if you notice: breathlessness at rest, chest pain, fainting or near-fainting, a persistently racing heart, or dizziness that doesn’t pass when you sit down. These don’t always mean something serious, but they’re worth a prompt check rather than waiting for your next visit.
Special situations that raise your risk
Some pregnancies start with the deck stacked toward anemia. You’re at higher risk if you’re carrying twins or more, had closely spaced pregnancies, or dealt with heavy periods before conceiving.
A vegetarian or vegan diet, a history of bariatric surgery, frequent vomiting from morning sickness, and teen pregnancy all raise the odds too. If any of these fit you, it’s worth flagging early so your provider can check iron stores before a shortfall sets in.
High RBC in Pregnancy: An Overlooked Signal
Nearly every article on pregnancy and red blood cells fixates on counts that run too low. A count that’s too high gets ignored, even though it occasionally carries useful information. Here’s the piece most pages skip.
Dehydration and morning sickness
The most common reason for an elevated RBC reading in pregnancy is plain dehydration. Lose fluid, and your plasma shrinks while the red cells crowd closer together, pushing the count up without any real change in the cells themselves.
Severe morning sickness with frequent vomiting is a classic trigger. Our lab partners report that a high reading often settles once a patient rehydrates, so the number is frequently a hydration story rather than a blood disorder.
Smoking, altitude, and rarer causes
Smoking and life at high altitude both push red cell production up, because the body compensates for thinner available oxygen. Rarely, a genuinely high count reflects a blood condition such as polycythemia, which calls for specialist evaluation.
Why an early high count can matter
There’s also a risk angle worth knowing. Research on blood composition through pregnancy found that high erythrocyte (red cell) levels in the first trimester were associated with a modestly higher chance of postpartum hemorrhage, while high levels in the third trimester were not, per a study on blood-count changes and PPH risk. One reading is no reason to panic, but it’s a reason your OB tracks the trend.
When a high count needs a closer look
Most high readings trace back to too little fluid, but a count that stays elevated after you’re well hydrated deserves follow-up. Persistent erythrocytosis can occasionally signal an oxygen-supply issue, a kidney condition, or a primary blood disorder.
Your provider may repeat the CBC, check your oxygen levels, or look at the other indices before deciding whether anything beyond hydration is going on. The goal isn’t to alarm you; one odd number is simply a prompt to look closer, not to worry.
How Doctors Test and Track Your RBC
You won’t be left to read these numbers alone. Prenatal care builds in checkpoints designed to catch trouble early, all using one familiar test.
The CBC and what it measures
The complete blood count (CBC) is the workhorse. Beyond the RBC count, it reports hemoglobin, hematocrit, and the red cell indices: MCV (cell size), MCH and MCHC (hemoglobin content), and RDW (variation in cell size).
Those indices are what let your doctor explain why a count is low. Small cells point toward iron deficiency, large cells suggest B12 or folate gaps, and a high RDW hints at more than one cause at work.
What each red cell index tells your doctor
Each letter on the panel earns its place. MCV gauges average cell size, MCH and MCHC measure how much hemoglobin each cell carries, and RDW captures how much your cell sizes vary from one to the next.
Read together, they sketch a quick portrait. Small, low-hemoglobin cells with a high RDW lean toward iron deficiency, while uniformly large cells suggest a B12 or folate gap. That pattern is how a single blood draw can point straight at a likely cause.
When screening happens
US guidelines on timing are clear and consistent. ACOG, the American Academy of Family Physicians, and the CDC recommend screening every pregnant patient for anemia at the first prenatal visit, with ACOG advising a repeat screen at 24 to 28 weeks of gestation.
That second check is placed deliberately near the hemodilution low point, so it catches anemia that develops as pregnancy advances. In testing booked through HealthCareOnTime, the 24-to-28-week window is the one we most often remind patients not to skip.
Reading your own results without panic
When portal results land, resist comparing every value against the non-pregnant range printed beside it. Check hemoglobin against the trimester-specific cutoffs, note whether you actually have symptoms, and bring your questions to your provider.
One note on fairness. ACOG advises against using different hemoglobin thresholds based on race, since observed differences in average levels reflect social and structural factors, not biology. One fair standard applies to everyone.
Raising Low RBC Safely: Iron, Diet, and Supplements
If your numbers do slip into true anemia, the fix is usually straightforward. Most cases come down to iron, with food and supplements pulling together. The figures below show why diet alone often falls short for US moms.
| Metric | Figure | Source |
| US anemia prevalence in pregnancy (2018 to 2023) | 25.6% | Obstetrics & Gynecology |
| Anemia at mid-pregnancy (22 to 30 weeks) | 24.5% | Obstetrics & Gynecology |
| Iron-deficiency share of pregnancy anemia | About 75% | Medscape clinical review |
| Iron RDA during pregnancy | 27 mg per day | NIH Office of Dietary Supplements |
| Extra iron a single pregnancy requires | About 1,000 mg | ACOG |
| US pregnant women below the dietary iron target | 83.8% | NIH Office of Dietary Supplements |
Iron-rich foods and smarter absorption
Food is the foundation. Strong US sources include lean red meat, poultry, and seafood (heme iron, which absorbs well), plus beans, lentils, tofu, spinach, and iron-fortified cereals (non-heme iron).
Absorption is half the battle. Pair plant-based iron with vitamin C (citrus, bell peppers, strawberries) to lift uptake, and keep iron-rich meals away from coffee, tea, and calcium-rich foods, which blunt it. These small timing tweaks often matter as much as the food itself.
A closer look at iron-rich US foods
Not all iron is created equal. Heme iron from animal foods absorbs at roughly 15% to 35%, while non-heme iron from plants lands closer to 2% to 20%, which is why pairings matter so much for plant-forward eaters.
Reliable US picks include lean beef, oysters, turkey, and chicken on the heme side, plus lentils, white beans, tofu, pumpkin seeds, spinach, and iron-fortified breakfast cereals on the plant side. Cooking acidic foods in a cast-iron pan can nudge your intake up a little too.
Supplement guidance that matches US recommendations
The iron RDA in pregnancy is 27 mg a day, yet a typical American diet delivers only about 15 mg, which is why the CDC recommends routine low-dose iron supplementation for most pregnant patients. Most prenatal vitamins already contain that 27 mg.
If you’re treating diagnosed iron-deficiency anemia, your provider may prescribe a higher therapeutic dose. Recent evidence suggests every-other-day dosing can work as well as daily dosing with fewer side effects like nausea and constipation, a tip our reviewers often share with patients who struggle to tolerate iron.
What not to do
More iron isn’t automatically better. The tolerable upper limit in pregnancy is 45 mg a day, and about 28% of US pregnant women already exceed it once food and supplements stack up, per NIH data. Megadosing on your own can cause real harm, so adjust iron only with your provider’s guidance.
RBC Levels After Delivery: The Postpartum Picture
Your red blood cells don’t stop changing once the baby arrives. Delivery brings blood loss, and the weeks that follow have their own pattern worth watching, especially if you were already anemic going into labor.
Blood loss at birth and early recovery
A typical vaginal birth involves some blood loss, and a cesarean usually more. For most women, the body rebuilds red cells over the following weeks as plasma volume settles back down and the marrow keeps producing.
If you started labor anemic or had heavier-than-usual bleeding, your count can dip further before it climbs. Many providers recheck hemoglobin after delivery when bleeding was significant, a step our patients are sometimes surprised to learn is routine.
Postpartum anemia and feeling drained
Postpartum anemia can deepen the exhaustion that already comes with a newborn, sometimes showing up as lingering fatigue, dizziness, or a low mood. Continuing iron after birth is a common recommendation when your stores ran low during pregnancy.
Iron needs while breastfeeding
The iron RDA actually drops during lactation to about 9 mg a day, lower than in pregnancy, because monthly periods usually pause. Even so, refilling depleted stores often takes months, so don’t be surprised if your provider keeps you on a supplement for a while.
When to call after birth
Reach out to your provider after delivery if you feel faint, your heart races with mild activity, you’re soaking through pads faster than expected, or the bone-deep tiredness simply isn’t easing. These can be signs your red cell count needs attention rather than just more rest.
Frequently Asked Questions
What is a normal RBC count during pregnancy?
Normal shifts by trimester. Common US reference ranges run about 3.42 to 4.55 million cells per microliter in the first trimester, 2.81 to 4.49 in the second, and 2.71 to 4.43 in the third. Counts sit lower than pre-pregnancy values because of natural blood dilution.
Why does my RBC drop in the second trimester?
Your plasma (blood’s liquid part) expands faster than your red cell mass, and this dilution peaks in the second trimester. The result is a lower RBC count, hemoglobin, and hematocrit. It’s called physiologic anemia and is a normal, expected part of a healthy pregnancy.
Is low RBC dangerous for my baby?
Mild dilutional anemia generally isn’t harmful. True anemia, especially untreated iron-deficiency anemia, is linked to higher risks of preterm birth and low birth weight. That’s why screening matters. Caught early, it usually responds well to iron, protecting both you and your baby.
What’s the difference between low RBC and anemia?
A low RBC flag often just reflects normal pregnancy dilution measured against non-pregnant ranges. Anemia is defined mainly by hemoglobin falling below trimester-specific cutoffs (under 11 g/dL in the first and third trimesters, under 10.5 in the second), often with symptoms.
What causes high RBC during pregnancy?
The most common cause is dehydration, which concentrates the blood and raises the count temporarily. Frequent vomiting from morning sickness, smoking, and high altitude can also elevate it. Rarely, a true blood disorder is responsible, which is why persistent high readings get evaluated.
How fast can I raise my red blood cells?
With iron supplementation for iron-deficiency anemia, many people see hemoglobin start rising within a couple of weeks, with a reticulocyte (young red cell) bump even sooner. Full recovery takes longer. Your provider typically rechecks levels about two to four weeks after starting treatment.
Which foods raise RBC during pregnancy?
Lean red meat, poultry, and seafood offer well-absorbed heme iron. Beans, lentils, tofu, spinach, and fortified cereals provide non-heme iron. Pair plant sources with vitamin C foods like citrus or bell peppers, and keep iron meals away from coffee, tea, and calcium for better absorption.
When is anemia screened during pregnancy?
US guidelines recommend a CBC at your first prenatal visit, ideally in the first trimester, and a repeat screen at 24 to 28 weeks. That second test is timed near the natural low point of your red cell counts, so it catches anemia that develops as pregnancy progresses.
Can I have iron deficiency without anemia?
Yes, and it’s common. Your iron stores can run low before your hemoglobin drops far enough to qualify as anemia. A ferritin test measures stored iron and can reveal early depletion. Treating it promptly helps prevent full iron-deficiency anemia later in pregnancy.
Do I need iron pills if my count is normal?
The CDC recommends routine low-dose iron (around 27 mg, the amount in most prenatal vitamins) for most pregnant patients, even without anemia, because dietary iron usually falls short. Some conditions like hemochromatosis are exceptions, so confirm your plan with your provider.
What RBC level is too low in pregnancy?
There’s no single magic number, since hemoglobin defines anemia more reliably than the RBC count alone. A hemoglobin below the trimester cutoff, a count well beneath the pregnancy reference range, or readings paired with symptoms all signal a level that needs evaluation and likely treatment.
When should I call my doctor about my count?
Call promptly if you have breathlessness at rest, chest pain, fainting, a persistently racing heart, or disruptive dizziness. Also reach out if you’re craving ice or non-food items, or if a lab result sits clearly below your trimester range. When in doubt, ask.
Medical disclaimer: This article is for general educational purposes and reflects current US clinical guidance from sources like the CDC, ACOG, and the NIH. It isn’t a substitute for personalized medical advice. Reference ranges vary slightly between labs, and your own targets depend on your health history. Always discuss your blood test results, symptoms, and any supplement or medication decisions with your obstetrician or healthcare provider.
References
- Centers for Disease Control and Prevention via USPSTF: Iron Deficiency and Iron Deficiency Anemia During Pregnancy, Screening and Supplementation
- NIH Office of Dietary Supplements: Dietary Supplements and Life Stages, Pregnancy
- Cleveland Clinic: Anemia During Pregnancy
- Obstetrics & Gynecology: Anemia During Pregnancy in a US Nationwide Cohort, 2018 to 2023
- American Journal of Clinical Nutrition: Hemoglobin Distributions and Prevalence of Anemia in a Multiethnic US Pregnant Population
- Medscape: Anemia and Thrombocytopenia in Pregnancy
- Perinatology.com: Red Blood Cell Count Reference Values in Pregnancy (Williams Obstetrics / Abbassi-Ghanavati)
- PMC: Postpartum Hemorrhage Risk and Blood Composition Changes Through Pregnancy





